Вам также может понравиться
- PEDIA Case 4.1. Dengue FeverДокумент10 страницPEDIA Case 4.1. Dengue Feverotartil_nimanОценок пока нет
- Pedia 1Документ8 страницPedia 1Jani MisterioОценок пока нет
- Case Write Up - Harmeet - Multinodular GoitreДокумент29 страницCase Write Up - Harmeet - Multinodular GoitreShalini Soorya71% (7)
- Acute Appendicitis: Surgical PostingДокумент8 страницAcute Appendicitis: Surgical PostingGraldoОценок пока нет
- Case Presentation - Acute GlomerulonephritisДокумент10 страницCase Presentation - Acute GlomerulonephritisRold Brio SosОценок пока нет
- Case Study On Stroke PatientДокумент2 страницыCase Study On Stroke PatientsparrowcrowОценок пока нет
- CR Piopneumothoraks Nicky FIXdДокумент62 страницыCR Piopneumothoraks Nicky FIXdPutri RahmawatiОценок пока нет
- Protocol - IM DyspneaДокумент7 страницProtocol - IM DyspneaTrisОценок пока нет
- Kasus Perdarahan Intrakranial Pada Bayi Baru LahirДокумент58 страницKasus Perdarahan Intrakranial Pada Bayi Baru LahirRechax Squad RezapawelloiОценок пока нет
- Cwu SurgeryДокумент16 страницCwu SurgeryAslah NabilahОценок пока нет
- CASE REPORT PiopneumothoraksДокумент9 страницCASE REPORT PiopneumothoraksAmriansyah PranowoОценок пока нет
- PP CaseДокумент48 страницPP CaseDany PrabowoОценок пока нет
- Case ReportДокумент22 страницыCase ReportAgus MahendraОценок пока нет
- Case Write-Up 1Документ16 страницCase Write-Up 1Zharif Fikri100% (3)
- Posting ElectiveДокумент7 страницPosting ElectiveThulasi tootsieОценок пока нет
- Case Report Ii.1 Identification Ii.3 Phisycal ExaminationДокумент10 страницCase Report Ii.1 Identification Ii.3 Phisycal ExaminationMasayu Mutiara UtiОценок пока нет
- Caseeeee Egaaa IrbasssДокумент27 страницCaseeeee Egaaa IrbasssIrbasMantiniSyaifulОценок пока нет
- 'Batangas Medical Center Case Report by PGI Carlos H. AcuñaДокумент7 страниц'Batangas Medical Center Case Report by PGI Carlos H. AcuñaCarlos H. AcuñaОценок пока нет
- Tuberculosis and Nephrotic Syndrome in A Child: Case ReportДокумент34 страницыTuberculosis and Nephrotic Syndrome in A Child: Case ReportAldo YustiantoОценок пока нет
- Presentation of Nephrotic Syndrome ICKAДокумент16 страницPresentation of Nephrotic Syndrome ICKABagas NovandyОценок пока нет
- Kasus Perdarahan Intrakranial Pada Bayi Baru LahirДокумент58 страницKasus Perdarahan Intrakranial Pada Bayi Baru LahirSilvia PAgitta TariganОценок пока нет
- Fakultas Kedokteran Universitas Nusa Cendana Kupang SMF Ilmu Penyakit Dalam Rsud Prof. W. Z. Johannes Kupang 2018Документ42 страницыFakultas Kedokteran Universitas Nusa Cendana Kupang SMF Ilmu Penyakit Dalam Rsud Prof. W. Z. Johannes Kupang 2018indahОценок пока нет
- Acute Appendicitis 3Документ8 страницAcute Appendicitis 3Aiman ArifinОценок пока нет
- CWU 1 SurgeryДокумент23 страницыCWU 1 SurgeryAmelia AkmarОценок пока нет
- CC 2 Mei 2017 PneumoniaДокумент37 страницCC 2 Mei 2017 PneumoniaAhimsa Yoga AninditaОценок пока нет
- Presentation of Nephrotic SyndromeДокумент15 страницPresentation of Nephrotic SyndromeBagas NovandyОценок пока нет
- MR GoutyДокумент25 страницMR GoutyArvindan SubramaniamОценок пока нет
- CFGVДокумент28 страницCFGVmyolie wuОценок пока нет
- AECOADДокумент7 страницAECOADAiman Arifin100% (1)
- Clinicalmeetingoriginal 161117192705Документ50 страницClinicalmeetingoriginal 1611171927057dbnf4stjyОценок пока нет
- Er Duty Report Rspad Gatot Soebroto Jakarta Wednesday, 20 JANUARY 2015Документ29 страницEr Duty Report Rspad Gatot Soebroto Jakarta Wednesday, 20 JANUARY 2015Faraida Jilzani ArsadОценок пока нет
- Case History: Personal DataДокумент5 страницCase History: Personal DataMohammed AhmedОценок пока нет
- Acute AppendicitisДокумент7 страницAcute AppendicitisAiman ArifinОценок пока нет
- SOAP NoteДокумент8 страницSOAP NoteAnonymous p0y5mmLQОценок пока нет
- Case Report: Left Pleural Efussion E.C. Lung Adenokarcinoma Stadium IvДокумент17 страницCase Report: Left Pleural Efussion E.C. Lung Adenokarcinoma Stadium IvAtsilah UlfahОценок пока нет
- Enterobiasis CaseДокумент4 страницыEnterobiasis CaseKimm Delos ReyesОценок пока нет
- Medical Report - PneumoniaeДокумент8 страницMedical Report - Pneumoniaenguyenhoavanchi2002Оценок пока нет
- CC 10 NOv 2017 ITPДокумент32 страницыCC 10 NOv 2017 ITPLilik NatasubrataОценок пока нет
- Pleural Effusion Ec Pulmonary TuberculosisДокумент45 страницPleural Effusion Ec Pulmonary TuberculosisYunny SafitriОценок пока нет
- Massive Left-Sided Pleural Effusion: and Normocytic Normochromic AnemiaДокумент25 страницMassive Left-Sided Pleural Effusion: and Normocytic Normochromic AnemiaDesita PermatasariОценок пока нет
- Unstable Angina With Underlying DyslipidaemiaДокумент9 страницUnstable Angina With Underlying DyslipidaemiaAiman ArifinОценок пока нет
- Case Write Up MedicineДокумент16 страницCase Write Up MedicineKamogelo MabotjaОценок пока нет
- DUTY REPORT Igd Ecy AbeДокумент21 страницаDUTY REPORT Igd Ecy AbeAsiah AbdillahОценок пока нет
- Case Presentation Acute GlomerulonephritisДокумент10 страницCase Presentation Acute Glomerulonephritisminangsung minangnengОценок пока нет
- Empyema ThoracisДокумент14 страницEmpyema ThoracisMara AbantoОценок пока нет
- Surgery 2 Case ReportДокумент12 страницSurgery 2 Case ReportElvis NgОценок пока нет
- Case Report III Internal MedicineДокумент12 страницCase Report III Internal MedicineGidu Said0% (1)
- Differential Diagnosispage of ValidationДокумент38 страницDifferential Diagnosispage of ValidationiinmsОценок пока нет
- Case - IUFDДокумент5 страницCase - IUFDMaris Sarline OpenianoОценок пока нет
- Peds Case 3Документ5 страницPeds Case 3Mohammed AhmedОценок пока нет
- CASE REPORT Dr. Arie Polim, SpOG FinalДокумент50 страницCASE REPORT Dr. Arie Polim, SpOG FinalpriskavkОценок пока нет
- Efusi Pleura Ec Ca ParuДокумент33 страницыEfusi Pleura Ec Ca ParuRahma Putri KinasihОценок пока нет
- Case 1 Pedia Henoch Schonlein PurpuraДокумент45 страницCase 1 Pedia Henoch Schonlein PurpuraJefferson Gumiran100% (1)
- Patient CaseДокумент9 страницPatient CaseMohamed AshrafОценок пока нет
- Discharge Summary JAGONOYДокумент6 страницDischarge Summary JAGONOYKirstie de LunaОценок пока нет
- Pih Case Study For PrintДокумент17 страницPih Case Study For Printfoxrivergate100% (1)
- CPC-Patho Version 6Документ20 страницCPC-Patho Version 6Bea SamonteОценок пока нет
- Group 2: Vaibhav Jain Kaliyannan Kayalvizhi Krishnamoorthy Srinath Kumar EswariДокумент35 страницGroup 2: Vaibhav Jain Kaliyannan Kayalvizhi Krishnamoorthy Srinath Kumar EswariZedd ZorïОценок пока нет
- CopdДокумент11 страницCopdBen Man Jun50% (2)
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicОт EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicРейтинг: 5 из 5 звезд5/5 (1)
- Kuliah Kesehatan MasyarakatДокумент13 страницKuliah Kesehatan MasyarakatDebby TamaraОценок пока нет
- Ileus MeconiumДокумент27 страницIleus MeconiumDebby TamaraОценок пока нет
- Ileus MeconiumДокумент27 страницIleus MeconiumDebby TamaraОценок пока нет
- MakalahДокумент36 страницMakalahDebby TamaraОценок пока нет
- Ante Sample ExamДокумент33 страницыAnte Sample ExamEric Matig-a EbradaОценок пока нет
- Clinmed 19 3 261bДокумент2 страницыClinmed 19 3 261bgevowo3277Оценок пока нет
- Disaster NursingДокумент52 страницыDisaster Nursingsweta100% (1)
- PNGIMR 40th Anniversary and ColloquiumДокумент116 страницPNGIMR 40th Anniversary and ColloquiumJamie CrossОценок пока нет
- Paper: Volodymyr A. Vinnikov and Oleg BelyakovДокумент12 страницPaper: Volodymyr A. Vinnikov and Oleg BelyakovMalik AzeemОценок пока нет
- Hyphema Uveitis AnteriorДокумент3 страницыHyphema Uveitis AnteriorMadelaineОценок пока нет
- New Zealand A To Z PathwayДокумент64 страницыNew Zealand A To Z PathwayTejas ShahОценок пока нет
- Pre Transfusion TestingДокумент57 страницPre Transfusion TestingDominic Bernardo100% (4)
- Assessing EarsДокумент11 страницAssessing EarsRhea Mae Visda RoaОценок пока нет
- Timeline For Lecture OnlyДокумент1 страницаTimeline For Lecture OnlyeyesontheskyОценок пока нет
- HEALTH TECHNOLOGY ASSESSMENT (Prelims)Документ17 страницHEALTH TECHNOLOGY ASSESSMENT (Prelims)Daddy Rules100% (1)
- The Use of Geriatric Assessment in The CommunityДокумент16 страницThe Use of Geriatric Assessment in The Communityhendra2darmawanОценок пока нет
- 61Документ205 страниц61Carlos HernándezОценок пока нет
- REFLEXOLOGYДокумент80 страницREFLEXOLOGYdonald duckОценок пока нет
- The Physician AssistantДокумент12 страницThe Physician AssistantThe Physician Assistant LifeОценок пока нет
- Short CV SidartawanДокумент2 страницыShort CV SidartawanHarry Margatama SaddhasagaraОценок пока нет
- Cytokines in Human HealthДокумент377 страницCytokines in Human Healthأبى جزاك الله خيراОценок пока нет
- Breast CancerДокумент53 страницыBreast CancerJCneriОценок пока нет
- AQUALIPOДокумент16 страницAQUALIPOAvalavenia Molina AbadОценок пока нет
- Atelectasis SymptomsДокумент4 страницыAtelectasis SymptomsMelDred Cajes BolandoОценок пока нет
- Classical Five-Element Acupuncture: Two More Powerful Treatment StrategiesДокумент10 страницClassical Five-Element Acupuncture: Two More Powerful Treatment StrategiesAОценок пока нет
- Pharmacovigilance For PanamaДокумент24 страницыPharmacovigilance For PanamamagicianchemistОценок пока нет
- Role of Nurse in ObstetricsДокумент6 страницRole of Nurse in ObstetricsSridevi DevarajОценок пока нет
- Intro To MPДокумент12 страницIntro To MPLeeShauran100% (2)
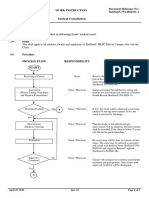
- WI-HSD-01 MALVAR Medical ConsultationДокумент2 страницыWI-HSD-01 MALVAR Medical ConsultationVictor BaluyotОценок пока нет
- TCCC Quick Reference Guide 2017Документ54 страницыTCCC Quick Reference Guide 2017https://www.t-medical.orgОценок пока нет
- Orthodontics-Gurkeerat Singh, 2nd EditionДокумент704 страницыOrthodontics-Gurkeerat Singh, 2nd Editionkeralaapple85% (34)
- AsepticДокумент3 страницыAsepticJen BallesterosОценок пока нет
- Shock ExamДокумент3 страницыShock ExamMilagros Fuertes Yosores100% (1)