Вам также может понравиться
- Learning IOM/HMD: Implications of the Institute of Medicine and Health & Medicine Division Reports for Nursing EducationОт EverandLearning IOM/HMD: Implications of the Institute of Medicine and Health & Medicine Division Reports for Nursing EducationРейтинг: 5 из 5 звезд5/5 (1)
- Textbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersОт EverandTextbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersОценок пока нет
- The Effects of Nurse Staffing On The Medical Surgical Unit Involving Patient Safety and Quality of CareДокумент13 страницThe Effects of Nurse Staffing On The Medical Surgical Unit Involving Patient Safety and Quality of Careapi-402644703Оценок пока нет
- Running Head: Health Care Issue Analysis 1Документ9 страницRunning Head: Health Care Issue Analysis 1api-393877273Оценок пока нет
- MAN-EMPOWERMENT - Strategies For Enhancing Autonomy and Control Over Nursing Practice PDFДокумент10 страницMAN-EMPOWERMENT - Strategies For Enhancing Autonomy and Control Over Nursing Practice PDFfriolan_cacliniОценок пока нет
- Nursing Bylaws 2009Документ30 страницNursing Bylaws 2009Silviana FassicaОценок пока нет
- Registered Nurse Shortage in Rural Healthcare SettingsДокумент9 страницRegistered Nurse Shortage in Rural Healthcare SettingsShelley KrumwiedeОценок пока нет
- Analysis On Policy HR 2581 - Selina DykesДокумент8 страницAnalysis On Policy HR 2581 - Selina Dykesapi-520664738Оценок пока нет
- ms1 Medication Errors PaperДокумент5 страницms1 Medication Errors Paperapi-417446716Оценок пока нет
- Nwnewgradprogramcl KbasakosДокумент1 страницаNwnewgradprogramcl Kbasakosapi-457168955Оценок пока нет
- Manager Interview PaperДокумент8 страницManager Interview Paperapi-301802746100% (2)
- 5 Storyboard (Contoh 1)Документ1 страница5 Storyboard (Contoh 1)RaniCianTarОценок пока нет
- Nursing ShortageДокумент16 страницNursing Shortageapi-240927368Оценок пока нет
- Staffing Nursing Management ReportДокумент54 страницыStaffing Nursing Management ReportTin MagbanuaОценок пока нет
- SBARДокумент6 страницSBARPutu Arik PebriyantiniОценок пока нет
- The Dangers of ComplacencyДокумент3 страницыThe Dangers of Complacencyegahmulia100% (2)
- Oral Care in ICUДокумент8 страницOral Care in ICUYani Va-Rhy100% (1)
- Resume-New GradДокумент1 страницаResume-New Gradapi-269394926Оценок пока нет
- Clinical Nursing Judgement PaperДокумент6 страницClinical Nursing Judgement Paperapi-401649778Оценок пока нет
- Pediatric TMC Cover LetterДокумент1 страницаPediatric TMC Cover Letterapi-383929607Оценок пока нет
- Pico PaperДокумент9 страницPico Paperapi-251822043Оценок пока нет
- Budgeting in HealthcareДокумент10 страницBudgeting in Healthcarepurity NgasiОценок пока нет
- Nurse StaffingДокумент29 страницNurse StaffingAi Åi100% (3)
- Determinants of HealthДокумент9 страницDeterminants of Healthapi-276860380Оценок пока нет
- Nur 4144 Quality Improvement PaperДокумент9 страницNur 4144 Quality Improvement Paperapi-370740810Оценок пока нет
- The Level Three TheoriesДокумент18 страницThe Level Three TheorieszhaeszОценок пока нет
- Ten Nursing TheoryДокумент13 страницTen Nursing TheoryleiОценок пока нет
- The Use of Turning and Repositioning Versus Pressure Redistributing Support Surfaces in The Prevention of Pressure UlcersДокумент14 страницThe Use of Turning and Repositioning Versus Pressure Redistributing Support Surfaces in The Prevention of Pressure UlcersLeena Salam100% (1)
- Quality Improvement ProjectДокумент6 страницQuality Improvement Projectapi-317112346Оценок пока нет
- My Capstone Project Reflection PaperДокумент10 страницMy Capstone Project Reflection Paperapi-223286633100% (1)
- Intravenous InsulinДокумент4 страницыIntravenous Insulingiseladelarosa2006Оценок пока нет
- Healthcare EthicsДокумент30 страницHealthcare EthicswetzelapulОценок пока нет
- Nurse Interview - Edited2Документ8 страницNurse Interview - Edited2Maina PeterОценок пока нет
- Toyin Fakus RPN ResumeДокумент2 страницыToyin Fakus RPN Resumeapi-283956153Оценок пока нет
- Nurs 440, Quality Improvement Process Paper, Fall 2014Документ8 страницNurs 440, Quality Improvement Process Paper, Fall 2014api-253664398Оценок пока нет
- FIU NGR 5110 Novice To Expert DiscussionДокумент3 страницыFIU NGR 5110 Novice To Expert Discussioninemjackson5553100% (1)
- Analysis On Nursing Competency StandardsДокумент6 страницAnalysis On Nursing Competency StandardsBijay PoudelОценок пока нет
- 2010 SWOT Harrison - Chapter5 Health Administration Press, 2010Документ7 страниц2010 SWOT Harrison - Chapter5 Health Administration Press, 2010Fernando NingunoОценок пока нет
- Nursing Philosophy and Professional Goals StatementДокумент7 страницNursing Philosophy and Professional Goals Statementapi-491461037Оценок пока нет
- Strengths Based NursingДокумент22 страницыStrengths Based NursingTHOHAROH0% (1)
- Multidisciplinary Team and Pharmacists Role in That TeamДокумент5 страницMultidisciplinary Team and Pharmacists Role in That TeamTimothy OgomaОценок пока нет
- 1I02 Clinical Nursing Practice Notes Week 3 Reflection (3 Parts)Документ39 страниц1I02 Clinical Nursing Practice Notes Week 3 Reflection (3 Parts)NTRisforthinkersОценок пока нет
- Nursing Practice ActДокумент74 страницыNursing Practice ActEmily DavisОценок пока нет
- Thesis (Noridja's Group)Документ31 страницаThesis (Noridja's Group)DenMarkSolivenMacniОценок пока нет
- Analyzing The Leadership Role of A Nurse ManagerДокумент7 страницAnalyzing The Leadership Role of A Nurse Managerapi-253808965100% (1)
- The Impact of The IOM Report On Nursing ScribdДокумент6 страницThe Impact of The IOM Report On Nursing ScribdLeonsa NatarenoОценок пока нет
- Nurse Manager InterviewДокумент7 страницNurse Manager Interviewapi-272621489Оценок пока нет
- Professional Meeting Reflection - GracДокумент3 страницыProfessional Meeting Reflection - Gracapi-540011183Оценок пока нет
- Nursing Philosophy Week 6Документ8 страницNursing Philosophy Week 6api-449137790Оценок пока нет
- Interprofessional InterviewДокумент5 страницInterprofessional Interviewapi-579620730Оценок пока нет
- Clinical Narrative Professional PortfolioДокумент6 страницClinical Narrative Professional Portfolioapi-336005635Оценок пока нет
- Medication Errors FinalДокумент5 страницMedication Errors Finalapi-379817190Оценок пока нет
- Regis NU668 Syllabus FA119Документ24 страницыRegis NU668 Syllabus FA119laotzu570Оценок пока нет
- Director Clinical Excellence Nursing in New York City Resume Sebrina FrinkДокумент2 страницыDirector Clinical Excellence Nursing in New York City Resume Sebrina FrinkSebrina FrinkОценок пока нет
- HealthWellness ResumesДокумент6 страницHealthWellness ResumesamanОценок пока нет
- Improving Nurse ResponsivenessДокумент13 страницImproving Nurse Responsivenessapi-446692943Оценок пока нет
- Laef BylawsДокумент15 страницLaef BylawsTibiОценок пока нет
- Sample Essay F5000FDДокумент7 страницSample Essay F5000FDAyshaОценок пока нет
- Observation Summary 2Документ5 страницObservation Summary 2api-493028287Оценок пока нет
- Critical Thinking Exercise - As A Change AgentДокумент8 страницCritical Thinking Exercise - As A Change AgentDennis Nabor Muñoz, RN,RMОценок пока нет
- Curriculum VitaeДокумент2 страницыCurriculum Vitaeapi-219741636Оценок пока нет
- Maternal Resuscitation DrillДокумент23 страницыMaternal Resuscitation Drillapi-219741636100% (2)
- Shoulder Dystocia ModuleДокумент18 страницShoulder Dystocia Moduleapi-219741636100% (1)
- Safe Staffing For Quality Care Act BrochureДокумент2 страницыSafe Staffing For Quality Care Act Brochureapi-219741636Оценок пока нет
- Msned Curriculum Group Project Final Edition 12-6-12 1Документ18 страницMsned Curriculum Group Project Final Edition 12-6-12 1api-219741636Оценок пока нет
- Enhancing Critical Thinking in Student Nurses Through ReflectionДокумент16 страницEnhancing Critical Thinking in Student Nurses Through Reflectionapi-219741636Оценок пока нет
- Research Proposal NCP Vs Reflective JournalДокумент30 страницResearch Proposal NCP Vs Reflective Journalapi-219741636Оценок пока нет
- Comparative Analysis Benner and Reflective PracticeДокумент25 страницComparative Analysis Benner and Reflective Practiceapi-219741636Оценок пока нет
- Annotated Bib Multidisciplinary Obstetric Emergency TrainingДокумент16 страницAnnotated Bib Multidisciplinary Obstetric Emergency Trainingapi-219741636Оценок пока нет
- Fall ProtectionДокумент4 страницыFall ProtectionnainaОценок пока нет
- PERSONAL PROTECTIVE EQUIPMENT Is Considered The Least Satisfactory Method in TheДокумент14 страницPERSONAL PROTECTIVE EQUIPMENT Is Considered The Least Satisfactory Method in TheAizen SousukeОценок пока нет
- Resume Vijeesh KumarДокумент3 страницыResume Vijeesh KumarunniОценок пока нет
- 72 516 PDFДокумент65 страниц72 516 PDFJITENDRA KUMAR SHARMAОценок пока нет
- Ergonomics Manual ToolsДокумент4 страницыErgonomics Manual ToolsZeeshan Bajwa100% (1)
- Positive Performance MeasurementДокумент42 страницыPositive Performance MeasurementSAYED100% (4)
- The Chinese EPCДокумент9 страницThe Chinese EPCAlfredo AstaОценок пока нет
- Permata Yang HilangДокумент19 страницPermata Yang Hilangeijam zainiОценок пока нет
- Hsems ManualДокумент211 страницHsems Manualronelbarafaeldiego100% (5)
- Attachment 3 - EHS RequirementsДокумент3 страницыAttachment 3 - EHS RequirementsAhmed Imtiaz RaoОценок пока нет
- MSDS - GulfSea Gear Oil@Документ4 страницыMSDS - GulfSea Gear Oil@Obydur RahmanОценок пока нет
- Chevron Regulatory Report Draft For Public CommentДокумент115 страницChevron Regulatory Report Draft For Public CommentKQED NewsОценок пока нет
- Health and Safety in ExcavationsДокумент65 страницHealth and Safety in Excavationsthirupathi9966Оценок пока нет
- Heat Stress ProcedureДокумент13 страницHeat Stress ProcedureKneekEy CastleОценок пока нет
- CV For ExampleДокумент4 страницыCV For ExampleArifin Ardhi100% (1)
- Acknowledgement: Mrs. Priya SrivastavaДокумент117 страницAcknowledgement: Mrs. Priya SrivastavaChandan SrivastavaОценок пока нет
- ACI Crack RepairДокумент6 страницACI Crack RepairelmerbarrerasОценок пока нет
- 28 - Scaffolding ProceduresДокумент17 страниц28 - Scaffolding ProceduresLalit Tomar100% (1)
- Safety Rules BrochureДокумент12 страницSafety Rules BrochureSuraj DeodathОценок пока нет
- Peo2 001Документ7 страницPeo2 001Jimmy Gray0% (1)
- Safety Documentation SystemДокумент165 страницSafety Documentation SystemPieter HerbstОценок пока нет
- 14 - Method Statements For Erection of Steel PDFДокумент1 страница14 - Method Statements For Erection of Steel PDFAbdul RahmanОценок пока нет
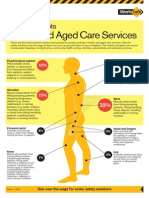
- Worksafe Victoria Injury Hot SpotsДокумент2 страницыWorksafe Victoria Injury Hot SpotsTucotakeda0% (1)
- Biolabs: Material Safety Data SheetДокумент3 страницыBiolabs: Material Safety Data SheetDarius DsouzaОценок пока нет
- Plumbing N1 Hands-On!Документ16 страницPlumbing N1 Hands-On!Future Managers Pty Ltd38% (8)
- Hazard Identification & ObjectivesДокумент2 страницыHazard Identification & Objectivesrajiv71Оценок пока нет
- Crown Battery Service Manual 101110Документ42 страницыCrown Battery Service Manual 101110Nelson Canteri100% (1)
- LOTOДокумент17 страницLOTOCris Angelo ValenciaОценок пока нет
- Health & Safety ManagementДокумент34 страницыHealth & Safety ManagementGovind Kumar SinghОценок пока нет