Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Immunization RecordДокумент4 страницыImmunization RecordVin BitzОценок пока нет
- 8 Abnormal BehaviorДокумент34 страницы8 Abnormal BehaviorRyanito MarquezОценок пока нет
- Immunization LectureДокумент32 страницыImmunization LectureMekdes ZewdeОценок пока нет
- Happy Vet Talk Ep 3 - Vaccine For CatsДокумент3 страницыHappy Vet Talk Ep 3 - Vaccine For CatsAditya Tri AnandaОценок пока нет
- AnnobibliДокумент7 страницAnnobibliapi-317692053Оценок пока нет
- 2021 08 21 07-03-33 AmДокумент1 страница2021 08 21 07-03-33 AmMohammad Masum HosenОценок пока нет
- Partial Record of Inventory Form of Vaccinated PaxДокумент18 страницPartial Record of Inventory Form of Vaccinated PaxDilg Asturias-CebuОценок пока нет
- Immunizing StudentsДокумент31 страницаImmunizing StudentsFedelyn Mae AcaylarОценок пока нет
- D.S.S AIIMS PREPRATION TEST SERIES MODEL PAPER - 8 SMALLPOX AND CHICKENPOXДокумент8 страницD.S.S AIIMS PREPRATION TEST SERIES MODEL PAPER - 8 SMALLPOX AND CHICKENPOXDr-Sanjay SinghaniaОценок пока нет
- Speaking C1 - Your Body Fights BackДокумент3 страницыSpeaking C1 - Your Body Fights Backne xemОценок пока нет
- Hepa B Vaccine Consent FormДокумент2 страницыHepa B Vaccine Consent FormKESLEY DELOS SANTOSОценок пока нет
- Chapter 4.3 Child Care and Services 2022Документ67 страницChapter 4.3 Child Care and Services 2022Nicole Sales DiazОценок пока нет
- Opv, Amv, Rota & Hib:, Side Effect and Home ManagementДокумент5 страницOpv, Amv, Rota & Hib:, Side Effect and Home Managementjohnlester_jlfОценок пока нет
- Viernes 3 - 2° Dosis SputnikДокумент48 страницViernes 3 - 2° Dosis SputnikSilvio GuanucoОценок пока нет
- Are Vaccines Up For DebateДокумент2 страницыAre Vaccines Up For DebateNiyah fairОценок пока нет
- Malaysian Covid-19 vaccination certificate detailsДокумент2 страницыMalaysian Covid-19 vaccination certificate detailsAlaghen VespanathanОценок пока нет
- SSC 55 Vaccine Antidote CombinationДокумент1 страницаSSC 55 Vaccine Antidote CombinationhimaОценок пока нет
- (DR) ONIMISI Anthony Baba & Isaac Sugar Ray.: RD THДокумент4 страницы(DR) ONIMISI Anthony Baba & Isaac Sugar Ray.: RD THBrian JollensОценок пока нет
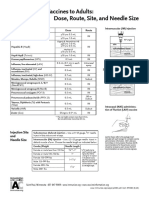
- Administering Vaccines To Adults: Dose, Route, Site, and Needle SizeДокумент1 страницаAdministering Vaccines To Adults: Dose, Route, Site, and Needle SizeAkashОценок пока нет
- Village vaccination recordsДокумент5 страницVillage vaccination recordsBbjvbjvОценок пока нет
- CertificateДокумент1 страницаCertificateShubham SinghОценок пока нет
- Package Insert - Varivax (Refrigerator)Документ14 страницPackage Insert - Varivax (Refrigerator)Jose Eduardo Oliva MarinОценок пока нет
- Immunization Record FormДокумент4 страницыImmunization Record FormLeonardo Zikri ArmandaОценок пока нет
- Certificate For COVID-19 Vaccination: Beneficiary DetailsДокумент1 страницаCertificate For COVID-19 Vaccination: Beneficiary DetailsCTM MURUGANОценок пока нет
- Primary One - Set 18Документ4 страницыPrimary One - Set 18Monydit santinoОценок пока нет
- ImmunisationДокумент58 страницImmunisationBharatBGОценок пока нет
- ShingrixДокумент6 страницShingrixMarcus YoonОценок пока нет
- Certificate For COVID-19 Vaccination: Beneficiary DetailsДокумент1 страницаCertificate For COVID-19 Vaccination: Beneficiary DetailsAman SinghОценок пока нет
- AEFIДокумент35 страницAEFIMisha ModiОценок пока нет
- Letter Urging Vaccines v1!7!27-21Документ3 страницыLetter Urging Vaccines v1!7!27-21USA TODAY NetworkОценок пока нет