Вам также может понравиться
- OBG Question DiscussionДокумент19 страницOBG Question DiscussionNesreden Jemal KedirОценок пока нет
- 1Документ10 страниц1drnsatyaprasadОценок пока нет
- Medical School Companion Obstetrics and Gynecology Practice Question BookОт EverandMedical School Companion Obstetrics and Gynecology Practice Question BookОценок пока нет
- Soal Usulan UnHas Juli 2019Документ25 страницSoal Usulan UnHas Juli 2019Ibnu SinaОценок пока нет
- Gynae & Obs Bcqs BookletДокумент58 страницGynae & Obs Bcqs BookletKiran Ayub100% (1)
- Latest Gynecology Multiple Choice Questions and Answers For PDFДокумент10 страницLatest Gynecology Multiple Choice Questions and Answers For PDFMohamed Al-zichrawy100% (1)
- Part I سنه القمله 2016Документ20 страницPart I سنه القمله 2016Aloah122346Оценок пока нет
- MCQs-Bank Obestetrics-Dr-Ahmed-Walid - Proffesor of Obs & Gyn - Benha Faculty of MedicineДокумент140 страницMCQs-Bank Obestetrics-Dr-Ahmed-Walid - Proffesor of Obs & Gyn - Benha Faculty of MedicineAhmed AnwarОценок пока нет
- Gynecological diagnoses and treatment tacticsДокумент19 страницGynecological diagnoses and treatment tacticssimi yОценок пока нет
- Obs and Gyn 6 Year Final Exam / 2012: A. PcosДокумент13 страницObs and Gyn 6 Year Final Exam / 2012: A. PcosNashaat H. AlshawabkehОценок пока нет
- Krok 2 2011 + AnswersДокумент69 страницKrok 2 2011 + AnswersKrish RoopunОценок пока нет
- مهم اسئلةДокумент19 страницمهم اسئلةnada elfarraОценок пока нет
- MCQДокумент41 страницаMCQBitu JaaОценок пока нет
- Normal flora, vaginal cysts, ovarian neoplasms, and cervical amputationДокумент14 страницNormal flora, vaginal cysts, ovarian neoplasms, and cervical amputationJha K SujitОценок пока нет
- DR Nadine Rev All (Samra's Edition)Документ313 страницDR Nadine Rev All (Samra's Edition)Cyril I.Makar100% (1)
- CMH Institute Gynecology Final Exam ReviewДокумент10 страницCMH Institute Gynecology Final Exam ReviewMunawarОценок пока нет
- 2022-23 OBG MMed 2 - 3btest 1 - KeyДокумент12 страниц2022-23 OBG MMed 2 - 3btest 1 - KeyKenneth ChandaОценок пока нет
- Gyne LE 2: Stage IVA Is Characterized byДокумент49 страницGyne LE 2: Stage IVA Is Characterized byĐinesh IlavarasanОценок пока нет
- Obstetrics GynecologyДокумент10 страницObstetrics GynecologyDiane UyОценок пока нет
- Operative Gyn MCQ PDFДокумент10 страницOperative Gyn MCQ PDFFentahun TadesseОценок пока нет
- كامل نساءДокумент181 страницаكامل نساءYasser ArefОценок пока нет
- CДокумент31 страницаCHambrian Wijaya100% (1)
- Common Sites of Cancer Metastasis and Management of Oncology CasesДокумент21 страницаCommon Sites of Cancer Metastasis and Management of Oncology Casesizat husseinОценок пока нет
- Antepartum HaemorrhageДокумент9 страницAntepartum HaemorrhageRCSCОценок пока нет
- IBQs & MCQsДокумент58 страницIBQs & MCQsskОценок пока нет
- MCQ Recall Paper - October 2001Документ33 страницыMCQ Recall Paper - October 2001dr_gentel19Оценок пока нет
- Obs I, 27 Desember 2007 Multiple ChoiceДокумент8 страницObs I, 27 Desember 2007 Multiple ChoiceLouis Hadiyanto100% (1)
- Clinical Case Presentation Anemia in Pregnancy: Ahmed Farrasyah Bin Mohd Kutubudin 071303511 Batch 24 Group A2Документ32 страницыClinical Case Presentation Anemia in Pregnancy: Ahmed Farrasyah Bin Mohd Kutubudin 071303511 Batch 24 Group A2kalpana gondipalliОценок пока нет
- Ain Shams MCQДокумент84 страницыAin Shams MCQمعتز حرارةОценок пока нет
- Medicbyte 1Документ115 страницMedicbyte 1Hengameh JavaheryОценок пока нет
- Jawaban 1Документ52 страницыJawaban 1Stefannus Wibisono100% (1)
- Infertility and gynecology case studiesДокумент24 страницыInfertility and gynecology case studiesChynthea ParamithaОценок пока нет
- Final Surgery RevisionДокумент195 страницFinal Surgery RevisionAbdulziz Al-jedaieОценок пока нет
- FCE OB GYN 2007 Male 2nd RoatationДокумент8 страницFCE OB GYN 2007 Male 2nd Roatationapi-3763146Оценок пока нет
- Obstetrics and Gynecology Practice QuestionsДокумент18 страницObstetrics and Gynecology Practice QuestionsSuzetteОценок пока нет
- Pregnancy quizДокумент8 страницPregnancy quizpoker011007Оценок пока нет
- Eu Test ObstrectiveДокумент12 страницEu Test ObstrectiveTanmay NainОценок пока нет
- Tes PanoramaДокумент57 страницTes Panoramamuttaqin95Оценок пока нет
- 2003 2008 MCQДокумент81 страница2003 2008 MCQIshola Segun SamuelОценок пока нет
- Ermp 2019 AnsДокумент32 страницыErmp 2019 AnsdrkefyalewtayeОценок пока нет
- Gynecologic Neoplasia Topic 1: Gestational Trophoblastic Neoplasia (GTD)Документ4 страницыGynecologic Neoplasia Topic 1: Gestational Trophoblastic Neoplasia (GTD)Elaine Marie Rendon PalmejarОценок пока нет
- Multiple ChoiceДокумент55 страницMultiple Choicetri ebtaОценок пока нет
- MCQ Year 3,26th July (Omega 7)Документ28 страницMCQ Year 3,26th July (Omega 7)Ammal Dzulfiqar Ismail100% (1)
- Group B Surgery QuestionsДокумент4 страницыGroup B Surgery QuestionsDarawan MirzaОценок пока нет
- Ats Menjawab Super Brankas Soal Unas 2020-2015Документ424 страницыAts Menjawab Super Brankas Soal Unas 2020-2015anton suponoОценок пока нет
- A) Atropine B) Adrenaline C) LidocaineДокумент8 страницA) Atropine B) Adrenaline C) LidocaineGalaleldin AliОценок пока нет
- The First Answer (A) Is Correct!Документ44 страницыThe First Answer (A) Is Correct!Cynthia GОценок пока нет
- Obstetrics MCQsДокумент12 страницObstetrics MCQsDeeksha BhardwajОценок пока нет
- 6th Year Obs&Gyne 2015Документ19 страниц6th Year Obs&Gyne 2015Rashed ShatnawiОценок пока нет
- MCQ Surgery 1Документ6 страницMCQ Surgery 1Abdallah GamalОценок пока нет
- General Medicine - Surgery IV YearДокумент40 страницGeneral Medicine - Surgery IV YearCynthia GОценок пока нет
- Mid Term Examination Papaer PEDSДокумент15 страницMid Term Examination Papaer PEDSHaslinОценок пока нет
- E. Prior Phenotypically Normal Infant Delivered at 34 Weeks Due To Spontaneous Preterm LaborДокумент10 страницE. Prior Phenotypically Normal Infant Delivered at 34 Weeks Due To Spontaneous Preterm LaborSK ASIF ALIОценок пока нет
- Clinico-Pathologic Conference 2015Документ43 страницыClinico-Pathologic Conference 2015Ezekiel ArtetaОценок пока нет
- Rev 4 - General Gynecology 2022Документ28 страницRev 4 - General Gynecology 2022Omar MohammedОценок пока нет
- January 2022 Exam (1) Answers Only Collected by EMLE NotesДокумент53 страницыJanuary 2022 Exam (1) Answers Only Collected by EMLE NotesIslam MohamedОценок пока нет
- Diagnosing Ectopic PregnancyДокумент5 страницDiagnosing Ectopic PregnancyDrPreeti Thakur ChouhanОценок пока нет
- Transposition of The Great ArteriesДокумент23 страницыTransposition of The Great Arterieswaseem mohammedОценок пока нет
- 5 Surgery PreTest Self-Assessment and Review 13th Edition-Pages-47-57,39-43Документ16 страниц5 Surgery PreTest Self-Assessment and Review 13th Edition-Pages-47-57,39-43Mae Rose Charlene MendozaОценок пока нет
- DR - Raja S Vignesh (Thoothukudi Medical College) in Hospital Care of Patient by NeurosurgeonДокумент25 страницDR - Raja S Vignesh (Thoothukudi Medical College) in Hospital Care of Patient by NeurosurgeonBrunoОценок пока нет
- Prof - Dr.Indumathy Santhanam (ICH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of ChildrenДокумент40 страницProf - Dr.Indumathy Santhanam (ICH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of ChildrenBrunoОценок пока нет
- Physiology and Pathology of Physical and Psychological StressДокумент60 страницPhysiology and Pathology of Physical and Psychological StressBrunoОценок пока нет
- Mrs. Sulochana (RGGGH) Current Status of Trauma Nursing in TNДокумент11 страницMrs. Sulochana (RGGGH) Current Status of Trauma Nursing in TNBrunoОценок пока нет
- Ms Ellaine Boo Role of Trauma NursingДокумент35 страницMs Ellaine Boo Role of Trauma NursingBrunoОценок пока нет
- DR - Rajesh CMO (RGGGH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of AdultsДокумент32 страницыDR - Rajesh CMO (RGGGH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of AdultsBruno100% (1)
- Prof DR Mark Fitzgerald Integrated In-Hospital Trauma Care - Building Blocks That Save LivesДокумент42 страницыProf DR Mark Fitzgerald Integrated In-Hospital Trauma Care - Building Blocks That Save LivesBrunoОценок пока нет
- DR - Joseph Mathew: Trauma Units and Team WorkДокумент39 страницDR - Joseph Mathew: Trauma Units and Team WorkBrunoОценок пока нет
- Prof DR Amit Gupta AITSC Trauma Registry & Trauma Quality Improvement in IndiaДокумент77 страницProf DR Amit Gupta AITSC Trauma Registry & Trauma Quality Improvement in IndiaBruno50% (2)
- TAEI NTRI WorkshopДокумент16 страницTAEI NTRI WorkshopBrunoОценок пока нет
- Prof Venkatesh Balasubramanian Current State Road Accident Database and Requirements For Integration of A Trauma RegistryДокумент37 страницProf Venkatesh Balasubramanian Current State Road Accident Database and Requirements For Integration of A Trauma RegistryBrunoОценок пока нет
- DR - Ramana Rao Pre-Hospital Services in Tamil NaduДокумент73 страницыDR - Ramana Rao Pre-Hospital Services in Tamil NaduBrunoОценок пока нет
- Hub and Spoke Model For STEMI Management - Tamil Nadu ModelДокумент16 страницHub and Spoke Model For STEMI Management - Tamil Nadu ModelBrunoОценок пока нет
- DR - Thambaiah (Cuddalore GH) in Hospital Care of Patients by OrthopaedicianДокумент36 страницDR - Thambaiah (Cuddalore GH) in Hospital Care of Patients by OrthopaedicianBruno100% (1)
- Prof DR Mark Fitzgerald What Is A Trauma System and Trauma System ComponentsДокумент36 страницProf DR Mark Fitzgerald What Is A Trauma System and Trauma System ComponentsBrunoОценок пока нет
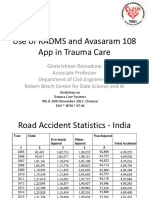
- Prof Gita Krishnan Ramadurai Use of RADAMS and 108 Avasaram App in Trauma CareДокумент21 страницаProf Gita Krishnan Ramadurai Use of RADAMS and 108 Avasaram App in Trauma CareBrunoОценок пока нет
- Neurosurgeon For A Social CauseДокумент55 страницNeurosurgeon For A Social CauseBrunoОценок пока нет
- TN Gazette 47 of 2013 Part VI Section 4Документ84 страницыTN Gazette 47 of 2013 Part VI Section 4BrunoОценок пока нет
- Prof DR Peter Cameron Measuring The Quality of Trauma Systems and In-Hospital Trauma CareДокумент46 страницProf DR Peter Cameron Measuring The Quality of Trauma Systems and In-Hospital Trauma CareBrunoОценок пока нет
- Mr. Dayanand Kataria, IAS Transport Commissioner Road Safety StatusДокумент25 страницMr. Dayanand Kataria, IAS Transport Commissioner Road Safety StatusBruno100% (1)
- NEET PG 2013 Rank List of Eligible CandidatesДокумент256 страницNEET PG 2013 Rank List of Eligible CandidatesBruno75% (8)
- DR - Darez Ahamed Vision For Tamil NaduДокумент6 страницDR - Darez Ahamed Vision For Tamil NaduBrunoОценок пока нет
- How Tamil Nadu Eradicated Organ SaleДокумент108 страницHow Tamil Nadu Eradicated Organ SaleBrunoОценок пока нет
- DR Joseph Mathew Designation of Trauma Hospitals in A Trauma SystemДокумент29 страницDR Joseph Mathew Designation of Trauma Hospitals in A Trauma SystemBrunoОценок пока нет
- Ian Patrick Pre-Hospital Systems in Australia Key Components of The Pre-Hospital System in Australia and Best Buys For Tamil NaduДокумент26 страницIan Patrick Pre-Hospital Systems in Australia Key Components of The Pre-Hospital System in Australia and Best Buys For Tamil NaduBrunoОценок пока нет
- Doctors' Role in Tackling Organ TradeДокумент70 страницDoctors' Role in Tackling Organ TradeBrunoОценок пока нет
- AR Rahman PDFДокумент405 страницAR Rahman PDFPitchai BalaОценок пока нет
- HMIS - Health Management Information System - Government of Tamil NaduДокумент12 страницHMIS - Health Management Information System - Government of Tamil NaduBruno100% (1)
- Why Tamil Nadu Model Works Better in Eradicating Organ SaleДокумент52 страницыWhy Tamil Nadu Model Works Better in Eradicating Organ SaleBrunoОценок пока нет
- Neurology, Neurosurgery MCQ PointsДокумент32 страницыNeurology, Neurosurgery MCQ PointsBruno86% (7)
- Legalization of Medical Marijuana in The Philippines H.R. 4477Документ2 страницыLegalization of Medical Marijuana in The Philippines H.R. 4477Joyce Ann Mauricio50% (2)
- HAAD Exam For Nurses Questions 2018Документ46 страницHAAD Exam For Nurses Questions 2018Asif Newaz100% (6)
- Hunsley & Mash (2007)Документ25 страницHunsley & Mash (2007)Raluca AdinaОценок пока нет
- !!!-MBS Skin Item Numbers Nov 2016Документ3 страницы!!!-MBS Skin Item Numbers Nov 2016abu ubaidahОценок пока нет
- Luliconazole Topical Cream MonographДокумент11 страницLuliconazole Topical Cream Monographdaizhussain004Оценок пока нет
- Physiotherapy For Quadriceps Tendon TearДокумент2 страницыPhysiotherapy For Quadriceps Tendon TearenadОценок пока нет
- MYOPIA REDUCTION... A View from the InsideДокумент6 страницMYOPIA REDUCTION... A View from the InsidePierre RodulfoОценок пока нет
- Report on Two Cases of Sialolithiasis and Literature ReviewДокумент4 страницыReport on Two Cases of Sialolithiasis and Literature Reviewmaharani spОценок пока нет
- Nasal Polyp Nasa Arsha Management Through Ayurveda A Single Case StudyДокумент4 страницыNasal Polyp Nasa Arsha Management Through Ayurveda A Single Case StudyEditor IJTSRDОценок пока нет
- Being Afraid: Everyday WorriesДокумент10 страницBeing Afraid: Everyday Worriesdina171279Оценок пока нет
- SpiritualityandGestalt AGestalt TranspersonalPerspectiveДокумент16 страницSpiritualityandGestalt AGestalt TranspersonalPerspectiveOlgaCanessa100% (1)
- Pathophysiology of A Anxiety Disorder PDFДокумент7 страницPathophysiology of A Anxiety Disorder PDFpragna novaОценок пока нет
- DR Miller Cost of Rhinoplasty InfographicДокумент1 страницаDR Miller Cost of Rhinoplasty Infographick8xcqsrxmqОценок пока нет
- Health & Nutrition Classification of FoodДокумент10 страницHealth & Nutrition Classification of Foodg20kpОценок пока нет
- Seminar On AsthmaДокумент27 страницSeminar On Asthmalumina.s100% (1)
- Shigella: The Organism/ToxinДокумент3 страницыShigella: The Organism/ToxinEduardo Ramirez LasoОценок пока нет
- Svolos Thomas - Introducing The SymptomДокумент5 страницSvolos Thomas - Introducing The SymptomManu GarcíaОценок пока нет
- USDOS ASPE Health Plan Contact and Claims InfoДокумент1 страницаUSDOS ASPE Health Plan Contact and Claims InfoEstrella Cotrina RojasОценок пока нет
- Ai 4 PlumpynutДокумент7 страницAi 4 PlumpynutdedrascОценок пока нет
- TramadolДокумент2 страницыTramadolJordanne EtisОценок пока нет
- Prenatal Fact SheetДокумент3 страницыPrenatal Fact Sheetapi-350949280Оценок пока нет
- Formulasi Tablet VaginalДокумент9 страницFormulasi Tablet VaginalnatinlalaОценок пока нет
- Ohi Graphic OrganizerДокумент1 страницаOhi Graphic Organizerapi-278298083Оценок пока нет
- Cervicogenic HeadacheДокумент32 страницыCervicogenic HeadacheasasakopОценок пока нет
- Personal Trainer Magazine PDFДокумент54 страницыPersonal Trainer Magazine PDFdixieakerszОценок пока нет
- Nursing Care Plan Deficiency of Fluid VolumeДокумент12 страницNursing Care Plan Deficiency of Fluid VolumefitrawatiarifuddinОценок пока нет
- OPD Schedule (02.08.2023)Документ5 страницOPD Schedule (02.08.2023)Private MineОценок пока нет
- Intro To Pharmacology Study GuideДокумент93 страницыIntro To Pharmacology Study GuideMichelle Morgan LongstrethОценок пока нет
- Ezzat PaperДокумент15 страницEzzat PaperMohamedAbdelmonaemОценок пока нет
- Section 1: Cellular AdaptationsДокумент30 страницSection 1: Cellular Adaptationshaddi awanОценок пока нет