Вам также может понравиться
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Government College of Engineering, Jalgaon: WWW - Gcoej.ac - inДокумент2 страницыGovernment College of Engineering, Jalgaon: WWW - Gcoej.ac - inchupchapОценок пока нет
- General Mathematics M1Документ26 страницGeneral Mathematics M1Ira Jane CaballeroОценок пока нет
- 102322641, Amanda Wetherall, EDU10024Документ7 страниц102322641, Amanda Wetherall, EDU10024Amanda100% (1)
- Aristotles Rational EmpiricismДокумент259 страницAristotles Rational EmpiricismPaoRobledoОценок пока нет
- 3.FIRST AID Snakebite LESSON PLANДокумент8 страниц3.FIRST AID Snakebite LESSON PLANdew2375% (4)
- Action Plan On Reading Intervention For Struggling Readers (Risr)Документ4 страницыAction Plan On Reading Intervention For Struggling Readers (Risr)Dennis De JesusОценок пока нет
- Klotz - The Keys To Heaven Also Open The Gates of Hell - Relativity and E mc2Документ19 страницKlotz - The Keys To Heaven Also Open The Gates of Hell - Relativity and E mc2EstimoОценок пока нет
- SEMINAR 08 Agreement and DisagreementДокумент5 страницSEMINAR 08 Agreement and Disagreementdragomir_emilia92Оценок пока нет
- (Edmond Bordeaux Szekely) Sexual Harmony (B-Ok - CC) PDFДокумент64 страницы(Edmond Bordeaux Szekely) Sexual Harmony (B-Ok - CC) PDFChristopher Carrillo100% (2)
- Carnap - Philosophy and Logical SyntaxДокумент10 страницCarnap - Philosophy and Logical SyntaxLorena PovedaОценок пока нет
- PHIL-IRI Manual 2018 Reorientation: Crisalie B. AnchetaДокумент76 страницPHIL-IRI Manual 2018 Reorientation: Crisalie B. AnchetaCrisalie ancheta100% (1)
- Fs 1-Episode 1Документ9 страницFs 1-Episode 1Louween Mendoza0% (1)
- 10 Mapeh ArtДокумент8 страниц10 Mapeh ArtMuhammad Amai-kurutОценок пока нет
- Soci1002 Unit 8 - 20200828Документ12 страницSoci1002 Unit 8 - 20200828YvanОценок пока нет
- NIT Recruitment RulesДокумент9 страницNIT Recruitment RulesTulasiram PatraОценок пока нет
- Detailed Lesson Plan in Mathematics Grade 3 Quarter Four Week Ten Day OneДокумент34 страницыDetailed Lesson Plan in Mathematics Grade 3 Quarter Four Week Ten Day OneJohn Paul Dela Peña86% (7)
- The Da Vinci Studio School of Creative EnterpriseДокумент32 страницыThe Da Vinci Studio School of Creative EnterpriseNHCollegeОценок пока нет
- Methods of TeachingДокумент11 страницMethods of TeachingnemesisОценок пока нет
- GCSE Computer Science Introduction To The Scheme WorkДокумент5 страницGCSE Computer Science Introduction To The Scheme WorkMujib AbdОценок пока нет
- Group Counseling Outline For Elementary Aged GirlsДокумент18 страницGroup Counseling Outline For Elementary Aged GirlsAllison Seal MorrisОценок пока нет
- The TKT Course Modules 1 2 and 3 2ndДокумент262 страницыThe TKT Course Modules 1 2 and 3 2ndEssential English CentreОценок пока нет
- ParaprofessionalДокумент2 страницыParaprofessionalapi-314847014Оценок пока нет
- Effective Management of Sales Force & Distribution ChannelsДокумент4 страницыEffective Management of Sales Force & Distribution Channelspkpratyush6305Оценок пока нет
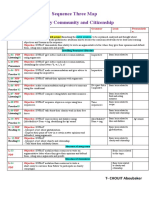
- CHOUIT Aboubaker MS4 Seq03 MapДокумент1 страницаCHOUIT Aboubaker MS4 Seq03 Mapthe rose of snow زهرة الثلج100% (1)
- 123 - Jan-Feb1947 - The Purpose of EducationДокумент2 страницы123 - Jan-Feb1947 - The Purpose of EducationBen LernerОценок пока нет
- New Teacher Orientation Day Classroom ManagementДокумент3 страницыNew Teacher Orientation Day Classroom Managementapi-248910805Оценок пока нет
- I3 Final Summary - External Review of Charter School ApplicationДокумент6 страницI3 Final Summary - External Review of Charter School ApplicationTrisha Powell CrainОценок пока нет
- O Level Maths P2 November 2012 Mark Scheme 21Документ6 страницO Level Maths P2 November 2012 Mark Scheme 21Kelvin MuzaОценок пока нет
- NVS PGT Result 2023 PDFДокумент57 страницNVS PGT Result 2023 PDFEr Arti Kamal BajpaiОценок пока нет
- Republic of The PhilippinesДокумент3 страницыRepublic of The PhilippinesIanx Valdez100% (1)