Вам также может понравиться
- Ucla Son Clinical Skills ChecklistДокумент31 страницаUcla Son Clinical Skills Checklistapi-247952145Оценок пока нет
- Clinical Nurse Leader Portfolio 1Документ7 страницClinical Nurse Leader Portfolio 1api-247952145Оценок пока нет
- Policy Issue - End of Life CareДокумент6 страницPolicy Issue - End of Life Careapi-247952145Оценок пока нет
- Chla-Portfolio ResumeДокумент2 страницыChla-Portfolio Resumeapi-247952145Оценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Access, Assessment & Continuity of CareДокумент14 страницAccess, Assessment & Continuity of CareamitОценок пока нет
- MediSafe Infinite PDFДокумент21 страницаMediSafe Infinite PDFNazim SalehОценок пока нет
- Curriculum Vitae Education UsmДокумент3 страницыCurriculum Vitae Education Usmapi-360825472Оценок пока нет
- Vice President or Executive Director or DirectorДокумент4 страницыVice President or Executive Director or Directorapi-77396522Оценок пока нет
- F. FeasibilityДокумент2 страницыF. Feasibilitypatricia gunioОценок пока нет
- To Identify Irrational Beliefs, Locus of Control, Quality of Work Life Among Nurses Working in Government and Corporate HospitalsДокумент8 страницTo Identify Irrational Beliefs, Locus of Control, Quality of Work Life Among Nurses Working in Government and Corporate HospitalsAnonymous CwJeBCAXpОценок пока нет
- A Patient's Bill of RightsДокумент4 страницыA Patient's Bill of RightsMark ElbenОценок пока нет
- Dr. Farzana Rashid Hossain - 2016 Women of DistinctionsДокумент64 страницыDr. Farzana Rashid Hossain - 2016 Women of DistinctionsFarzana Rashid Hossain, MDОценок пока нет
- Cover Letter ExampleДокумент2 страницыCover Letter ExampleChristina VongОценок пока нет
- Final Reflective StatementДокумент4 страницыFinal Reflective StatementPham KarinaОценок пока нет
- Health InsuranceДокумент9 страницHealth InsurancetceterexОценок пока нет
- Hospital Management SolutionДокумент4 страницыHospital Management SolutionsomyaОценок пока нет
- Obm752 Hospital Management QBДокумент43 страницыObm752 Hospital Management QBParanthaman GОценок пока нет
- Improving Hospital Performance and Productivity With The Balanced Scorecard - 2Документ22 страницыImproving Hospital Performance and Productivity With The Balanced Scorecard - 2Yunita Soraya HusinОценок пока нет
- Ppg-Gdch-Nur-42 Policy On Patient IdentificationДокумент7 страницPpg-Gdch-Nur-42 Policy On Patient IdentificationKenny JosefОценок пока нет
- SOP FinalДокумент7 страницSOP FinalsabaОценок пока нет
- Cover Letter ChlaДокумент1 страницаCover Letter Chlaapi-405154325Оценок пока нет
- Test 14Документ5 страницTest 14MH GamingОценок пока нет
- مشروع ادارة مستشفىДокумент130 страницمشروع ادارة مستشفىboothoОценок пока нет
- Role of Pharmacist in Reducing Healthcare CostsДокумент8 страницRole of Pharmacist in Reducing Healthcare CostsAnsar MushtaqОценок пока нет
- Hailey Carr Hughes ResumeДокумент2 страницыHailey Carr Hughes Resumeapi-533884212Оценок пока нет
- ResourcesДокумент104 страницыResourcesAbdoul Hakim BeyОценок пока нет
- Medical Services and ManagementДокумент17 страницMedical Services and ManagementjohnОценок пока нет
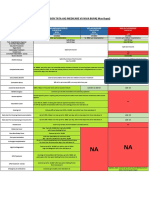
- Comparison Tata Aig Medicare Vs Niva BupaДокумент1 страницаComparison Tata Aig Medicare Vs Niva BupaTikekar ShubhamОценок пока нет
- Nawab Bugti AgreementДокумент6 страницNawab Bugti AgreementYounas BugtiОценок пока нет
- Annex A - Self-Assessment Tool For Proposed EPCB Health Facilities PDFДокумент5 страницAnnex A - Self-Assessment Tool For Proposed EPCB Health Facilities PDFCora Mendoza100% (1)
- PDFДокумент245 страницPDFSunil SewakОценок пока нет
- Enhanced E-R Model and Business RulesДокумент20 страницEnhanced E-R Model and Business RulesAbdirisak Mohamud0% (1)
- Vignette 1. Concepts of L&MДокумент4 страницыVignette 1. Concepts of L&MJohn Lyndon SayongОценок пока нет
- Philippine Health CareДокумент8 страницPhilippine Health CareCarl Mark Vincent BabasoroОценок пока нет