Вам также может понравиться
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Christian MinistriesДокумент23 страницыChristian MinistriesAnonymous 2Fx1dyОценок пока нет
- Aruba SD-WAN Professional Assessment Aruba SD-WAN Professional AssessmentДокумент2 страницыAruba SD-WAN Professional Assessment Aruba SD-WAN Professional AssessmentLuis Rodriguez100% (1)
- Inverse VariationДокумент4 страницыInverse VariationSiti Ida MadihaОценок пока нет
- Unit IV. Communication in Pharmacy Practice PDFДокумент54 страницыUnit IV. Communication in Pharmacy Practice PDFGeannea Mae LeañoОценок пока нет
- Tline Training Periodizaton Schedule PDFДокумент2 страницыTline Training Periodizaton Schedule PDFKolekade-Mattandkira AckerОценок пока нет
- Tline Poinsettia Tracker PDFДокумент1 страницаTline Poinsettia Tracker PDFKolekade-Mattandkira AckerОценок пока нет
- Tline Poinsettia TrackerДокумент1 страницаTline Poinsettia TrackerKolekade-Mattandkira AckerОценок пока нет
- Tline Feet-to-Fingertips Weight Training PDFДокумент1 страницаTline Feet-to-Fingertips Weight Training PDFKolekade-Mattandkira AckerОценок пока нет
- Tline In-Season Pitching PDFДокумент1 страницаTline In-Season Pitching PDFKolekade-Mattandkira AckerОценок пока нет
- Tline Warm-Up, Cool-Down and Flexibility PDFДокумент1 страницаTline Warm-Up, Cool-Down and Flexibility PDFKolekade-Mattandkira AckerОценок пока нет
- Tline Pitcing Program PDFДокумент6 страницTline Pitcing Program PDFKolekade-Mattandkira AckerОценок пока нет
- PS Fall Ball Standings 2013Документ1 страницаPS Fall Ball Standings 2013Kolekade-Mattandkira AckerОценок пока нет
- A's Hitting 2013Документ2 страницыA's Hitting 2013Kolekade-Mattandkira AckerОценок пока нет
- Tline Anaerobic Endurance Training PDFДокумент1 страницаTline Anaerobic Endurance Training PDFKolekade-Mattandkira AckerОценок пока нет
- TLine PoinsettiasДокумент1 страницаTLine PoinsettiasKolekade-Mattandkira AckerОценок пока нет
- JV BracketДокумент1 страницаJV BracketKolekade-Mattandkira AckerОценок пока нет
- Thurston County Baseball PDFДокумент1 страницаThurston County Baseball PDFKolekade-Mattandkira AckerОценок пока нет
- Tline Strenght and Power Training PDFДокумент9 страницTline Strenght and Power Training PDFKolekade-Mattandkira AckerОценок пока нет
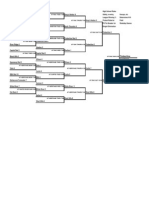
- Varsity BracketДокумент3 страницыVarsity BracketKolekade-Mattandkira AckerОценок пока нет
- PS Fall Ball Schedule 2013Документ1 страницаPS Fall Ball Schedule 2013Kolekade-Mattandkira AckerОценок пока нет
- PSCL Hawaii Camp FormДокумент1 страницаPSCL Hawaii Camp FormKolekade-Mattandkira AckerОценок пока нет
- Silvers Hitting 2013Документ2 страницыSilvers Hitting 2013Kolekade-Mattandkira AckerОценок пока нет
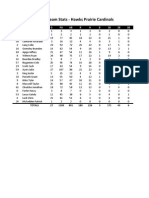
- Cards Hitting 2013Документ2 страницыCards Hitting 2013Kolekade-Mattandkira AckerОценок пока нет
- Saints Pitching 2013Документ2 страницыSaints Pitching 2013Kolekade-Mattandkira AckerОценок пока нет
- Silvers Pitching 2013Документ2 страницыSilvers Pitching 2013Kolekade-Mattandkira AckerОценок пока нет
- Cards Pitching 2013Документ2 страницыCards Pitching 2013Kolekade-Mattandkira AckerОценок пока нет
- A's Pitching 2013Документ2 страницыA's Pitching 2013Kolekade-Mattandkira AckerОценок пока нет
- Linx Hitting 2013Документ2 страницыLinx Hitting 2013Kolekade-Mattandkira AckerОценок пока нет
- Fathers Day Umpire Schedule 2013Документ2 страницыFathers Day Umpire Schedule 2013Kolekade-Mattandkira AckerОценок пока нет
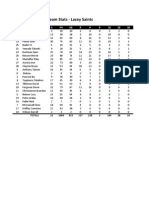
- Saints Hitting 2013Документ2 страницыSaints Hitting 2013Kolekade-Mattandkira AckerОценок пока нет
- Brewers Hitting 2013Документ2 страницыBrewers Hitting 2013Kolekade-Mattandkira AckerОценок пока нет
- Brewers Pitching 2013Документ2 страницыBrewers Pitching 2013Kolekade-Mattandkira AckerОценок пока нет
- Linx Pitching 2013Документ2 страницыLinx Pitching 2013Kolekade-Mattandkira AckerОценок пока нет
- The Ideology of DurationДокумент7 страницThe Ideology of DurationDave BeechОценок пока нет
- 1231Документ7 страниц1231Mervinlloyd Allawan BayhonОценок пока нет
- Cambridge Primary Parent Guide 2022Документ20 страницCambridge Primary Parent Guide 2022Dana SobhОценок пока нет
- Dully Filled Application FormДокумент2 страницыDully Filled Application FormMd Abdullah al QafiОценок пока нет
- Rizal As A Student (Summary)Документ5 страницRizal As A Student (Summary)Meimei FenixОценок пока нет
- Performance Management & ApraisalДокумент22 страницыPerformance Management & ApraisalKaustubh Barve0% (1)
- Shiela Mae S. Espina: ObjectiveДокумент2 страницыShiela Mae S. Espina: ObjectiveJude Bon AlbaoОценок пока нет
- Lista Manuale Macmillan Aprobate Şi Recomandate: Nr. Crt. Manual Level Aprobat MECT Clasa L1 L2 L3Документ4 страницыLista Manuale Macmillan Aprobate Şi Recomandate: Nr. Crt. Manual Level Aprobat MECT Clasa L1 L2 L3Cerasela Iuliana PienoiuОценок пока нет
- Final Exam b2 Answer SheetДокумент2 страницыFinal Exam b2 Answer SheetTolga ÖzcanОценок пока нет
- I.K.Gujral Punjab Technical University, Jalandhar: Jalandhar-Kapurthala Highway, JalandharДокумент1 страницаI.K.Gujral Punjab Technical University, Jalandhar: Jalandhar-Kapurthala Highway, JalandharManoj KumarОценок пока нет
- Conduct Surveysobservations ExperimentДокумент20 страницConduct Surveysobservations ExperimentkatecharisseaОценок пока нет
- ACADEMIC MANUAL - National Institute of Fashion TechnologyДокумент455 страницACADEMIC MANUAL - National Institute of Fashion TechnologyRalucaFlorentinaОценок пока нет
- Spanish PoemsДокумент22 страницыSpanish PoemskaiserjhinkzОценок пока нет
- 09 Bloom Gardner Matrix Example 2009Документ2 страницы09 Bloom Gardner Matrix Example 2009Ellen Jaye BensonОценок пока нет
- Traditional Lesson Plan 2nd QuarterДокумент4 страницыTraditional Lesson Plan 2nd QuarterHappy Delos Reyes Dela TorreОценок пока нет
- 200 Sanskrit Terms GRДокумент12 страниц200 Sanskrit Terms GRUwe HeimОценок пока нет
- Amherst Schools Staff Salaries 2012Документ17 страницAmherst Schools Staff Salaries 2012Larry KelleyОценок пока нет
- Name of Student: - Prefinal Assignment No.1 Course/Year/Section: - Date SubmittedДокумент2 страницыName of Student: - Prefinal Assignment No.1 Course/Year/Section: - Date SubmittedJericho GofredoОценок пока нет
- Delta Theta Book of RecordsДокумент398 страницDelta Theta Book of RecordsareyoubeefinОценок пока нет
- Children Songs As MediaДокумент13 страницChildren Songs As MediaOkta Eldi SurahmanОценок пока нет
- Human Rights Chap 6-9Документ14 страницHuman Rights Chap 6-9Lucky VastardОценок пока нет
- Final Moot Court Competition Rules of ProcedureДокумент4 страницыFinal Moot Court Competition Rules of ProcedureAmsalu BelayОценок пока нет
- HEE Topol Review 2019Документ53 страницыHEE Topol Review 2019Roger SenОценок пока нет
- Herbart SpencerДокумент32 страницыHerbart SpencerMohit PuriОценок пока нет
- PCR 271Документ205 страницPCR 271mztayyabОценок пока нет
- ZGE 4301 CSAH - M10 Activity No. 1 FT Climate ChangeДокумент10 страницZGE 4301 CSAH - M10 Activity No. 1 FT Climate ChangeMark Joshua PasicolanОценок пока нет