Вам также может понравиться
- Hyperbilirubinemia Teaching PlanДокумент2 страницыHyperbilirubinemia Teaching Planapi-25291041167% (3)
- Anastacio Wic FlyerДокумент2 страницыAnastacio Wic Flyerapi-252910411Оценок пока нет
- Mastitis Teaching PlanДокумент2 страницыMastitis Teaching Planapi-252910411Оценок пока нет
- Anastacio Slo Ethics n220Документ4 страницыAnastacio Slo Ethics n220api-252910411Оценок пока нет
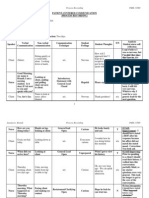
- 360 Process Recording TemplateДокумент13 страниц360 Process Recording Templateapi-252910411100% (9)
- Concept Map Care PlanДокумент5 страницConcept Map Care Planapi-252910411Оценок пока нет
- Concept MapДокумент1 страницаConcept Mapapi-252910411Оценок пока нет
- Capstone Concept MapДокумент1 страницаCapstone Concept Mapapi-252910411Оценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Introduction To Criminal Justice 4th Edition Bohm Test BankДокумент28 страницIntroduction To Criminal Justice 4th Edition Bohm Test BankArianaDiazsityz100% (14)
- What Is The Status of Special Education Program in The PhilippinesДокумент5 страницWhat Is The Status of Special Education Program in The PhilippinesJohn Kevin ANDRADE100% (7)
- Lesson 20 - The Purposes of PunishmentДокумент14 страницLesson 20 - The Purposes of Punishmentapi-249423644Оценок пока нет
- 006 People v. Honrada AnicetoДокумент2 страницы006 People v. Honrada AnicetoGTОценок пока нет
- Wendall Wallace - Is Incarceration The Best Method For Altering The Life Trajectory of Juvenile Offenders in Trinidad and TobagoДокумент28 страницWendall Wallace - Is Incarceration The Best Method For Altering The Life Trajectory of Juvenile Offenders in Trinidad and TobagoKamille CapiathaОценок пока нет
- Prefatory StatementДокумент2 страницыPrefatory StatementAko Si CrokieОценок пока нет
- RDL Introduction STEM - SanchezДокумент3 страницыRDL Introduction STEM - SanchezErik Maximus SarmientoОценок пока нет
- Sexual HarrasmentДокумент13 страницSexual HarrasmentFaisal SandhuОценок пока нет
- DocumentДокумент18 страницDocumentHarsh DubeyОценок пока нет
- Securing Children's Rights: Childreach International Strategy 2013-16Документ13 страницSecuring Children's Rights: Childreach International Strategy 2013-16Childreach InternationalОценок пока нет
- Democratic Awareness Through Legal Literacy-SEC BA Prog Sem 5 2020 - Khushboo VermaДокумент4 страницыDemocratic Awareness Through Legal Literacy-SEC BA Prog Sem 5 2020 - Khushboo VermaShahnawaz AkramОценок пока нет
- Gender and Society : "The Safe Space Kit:Guide To Being An Ally To LGBT Students"Документ2 страницыGender and Society : "The Safe Space Kit:Guide To Being An Ally To LGBT Students"Justine MangubatОценок пока нет
- GENDERДокумент3 страницыGENDERRuinz SsellОценок пока нет
- Gender InequalityДокумент2 страницыGender InequalityIness KhattabiОценок пока нет
- CriminologyДокумент12 страницCriminologyaditya vermaОценок пока нет
- Peoplevs AlipitДокумент2 страницыPeoplevs Alipitlleiryc7Оценок пока нет
- DILG VAWC FormДокумент5 страницDILG VAWC FormMah Jane Divina100% (1)
- Colorado CPS - Family Risk Assessment FormДокумент3 страницыColorado CPS - Family Risk Assessment FormRick ThomaОценок пока нет
- Adult BullyingДокумент3 страницыAdult BullyingLeonte ȘtirbuОценок пока нет
- Anti Sex EducationДокумент2 страницыAnti Sex EducationMartinОценок пока нет
- Gender-Based Violence: Survivor, Victim, Perpetrator, and Human RightsДокумент9 страницGender-Based Violence: Survivor, Victim, Perpetrator, and Human RightsEdriel Daquioag100% (1)
- Reviewer Crim 3 FinalsДокумент6 страницReviewer Crim 3 FinalsMaria Rafaella P. DadoОценок пока нет
- Rights of Persons With DisabilitiesДокумент15 страницRights of Persons With DisabilitiesAnkita DashОценок пока нет
- Bar Matter No 2502-Reforms For The 2012 Bar ExaminationsДокумент2 страницыBar Matter No 2502-Reforms For The 2012 Bar Examinationsgeorge_castaneda2013Оценок пока нет
- Memo For: All Students From: CAC Dean RE: CAC Policy On PlagiarismДокумент1 страницаMemo For: All Students From: CAC Dean RE: CAC Policy On PlagiarismIsaiah Emmanuel SuguitanОценок пока нет
- Case Filed in Court Result in Injustice and MistrialДокумент2 страницыCase Filed in Court Result in Injustice and MistrialAndrea GonzalesОценок пока нет
- SC 1325 Philippines Policies or Legislations That Manifest ComplianceДокумент5 страницSC 1325 Philippines Policies or Legislations That Manifest ComplianceEzra gambicanОценок пока нет
- GHHHHДокумент9 страницGHHHHSorina CalinОценок пока нет
- Factors Influencing Students Enrollment & Dropout of Private UniversityДокумент3 страницыFactors Influencing Students Enrollment & Dropout of Private UniversityTaseen AhmeedОценок пока нет
- CHYS 3P24 Lecture 8Документ3 страницыCHYS 3P24 Lecture 8Amanda ScottОценок пока нет