Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
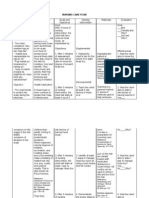
- Patient care and discharge planДокумент2 страницыPatient care and discharge planBryan Carmona100% (1)
- Oral Versus Topical NSAIDs in Rheumatic DiseasesДокумент21 страницаOral Versus Topical NSAIDs in Rheumatic DiseasesAnonymous so6ZnlKywОценок пока нет
- Enteral Feeding Nursing Care PlanДокумент2 страницыEnteral Feeding Nursing Care PlanChebz Zy0% (1)
- PediculosisДокумент3 страницыPediculosisDarkCeades50% (4)
- Pasion ThesisДокумент55 страницPasion ThesisMagiePasion100% (1)
- Case Osteoarthritis NewДокумент33 страницыCase Osteoarthritis NewQueenie P. Manalo67% (3)
- Case Log TotalsДокумент2 страницыCase Log Totalsapi-247959633Оценок пока нет
- Leeimrt 3Документ3 страницыLeeimrt 3api-247490129Оценок пока нет
- DaleaaffectiveevlsДокумент30 страницDaleaaffectiveevlsapi-247959633Оценок пока нет
- Nwsra PaperДокумент3 страницыNwsra Paperapi-247959633Оценок пока нет
- Daleaconformal 17Документ3 страницыDaleaconformal 17api-247959633Оценок пока нет
- LeebrachycompsДокумент3 страницыLeebrachycompsapi-247490129Оценок пока нет
- DaleaelectroncompДокумент2 страницыDaleaelectroncompapi-247959633Оценок пока нет
- Budget ActivityДокумент2 страницыBudget Activityapi-247490129Оценок пока нет
- Daleasummary - Evaluations From Anne MarieДокумент11 страницDaleasummary - Evaluations From Anne Marieapi-247959633Оценок пока нет
- Activity - Week 4-Case Study-Cpt CodesДокумент2 страницыActivity - Week 4-Case Study-Cpt Codesapi-247959633Оценок пока нет
- 3d SBRT Lung Case StudyДокумент11 страниц3d SBRT Lung Case Studyapi-247959633Оценок пока нет
- Relay For LifeДокумент3 страницыRelay For Lifeapi-247959633Оценок пока нет
- Medical Radiation Dosimetrist - UicДокумент4 страницыMedical Radiation Dosimetrist - Uicapi-247959633Оценок пока нет
- Sample BudgetДокумент6 страницSample Budgetapi-247959633Оценок пока нет
- Adriana Final 1Документ15 страницAdriana Final 1api-247959633Оценок пока нет
- Conferences SpringsummerДокумент6 страницConferences Springsummerapi-247959633Оценок пока нет
- Hall-2009 Article-Week 2 ArticleДокумент15 страницHall-2009 Article-Week 2 Articleapi-247959633Оценок пока нет
- Dalea Eport-Summary From Anne MarieДокумент3 страницыDalea Eport-Summary From Anne Marieapi-247959633Оценок пока нет
- 2014 CnsassignmentfinalДокумент1 страница2014 Cnsassignmentfinalapi-247959633Оценок пока нет
- ReferencesДокумент1 страницаReferencesapi-247959633Оценок пока нет
- Mentoring PaperДокумент5 страницMentoring Paperapi-247959633Оценок пока нет
- April Case StudyДокумент12 страницApril Case Studyapi-247959633Оценок пока нет
- Parotid LabДокумент3 страницыParotid Labapi-237266632Оценок пока нет
- Conferences SpringsummerДокумент6 страницConferences Springsummerapi-247959633Оценок пока нет
- Timelog-Spring SemesterДокумент12 страницTimelog-Spring Semesterapi-247959633Оценок пока нет
- Relay For LifeДокумент3 страницыRelay For Lifeapi-247959633Оценок пока нет
- Conferences-Summer SemДокумент3 страницыConferences-Summer Semapi-247959633Оценок пока нет
- March Case StudyДокумент9 страницMarch Case Studyapi-247959633Оценок пока нет
- Ama Challenge 2012Документ3 страницыAma Challenge 2012api-174496267Оценок пока нет
- February Case StudyДокумент10 страницFebruary Case Studyapi-247959633Оценок пока нет
- A Placebo-Controlled Test of Cognitive-Behavioral Therapy For Comorbid Insomnia in Older AdultsДокумент11 страницA Placebo-Controlled Test of Cognitive-Behavioral Therapy For Comorbid Insomnia in Older Adultssilvia dwi puspitaОценок пока нет
- SAFERamp - Whe-2314-09Документ3 страницыSAFERamp - Whe-2314-09608943Оценок пока нет
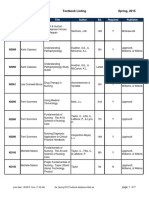
- BFLSON Course Textbook ListingДокумент7 страницBFLSON Course Textbook ListingWina ViqaОценок пока нет
- ERCP ExplainedДокумент4 страницыERCP ExplainedMichelle TamorОценок пока нет
- Or JournalДокумент5 страницOr JournalEchanique, James F.Оценок пока нет
- Andre Hannah NursingresumeДокумент1 страницаAndre Hannah Nursingresumeapi-450112281Оценок пока нет
- Rhopalurus Junceus: and The Treatment of CancerДокумент17 страницRhopalurus Junceus: and The Treatment of CancerAmalia Tri UtamiОценок пока нет
- Super Arrow Flex Sheath - Brochure - EN PDFДокумент3 страницыSuper Arrow Flex Sheath - Brochure - EN PDFbiomedical_com_brОценок пока нет
- StaphylococciДокумент25 страницStaphylococcichikitsakОценок пока нет
- Or-Indicator Measure Profile-Kpi-6.4 Day Surgery Conversion To AdmissionДокумент2 страницыOr-Indicator Measure Profile-Kpi-6.4 Day Surgery Conversion To Admissionangeli punoОценок пока нет
- Evans Shianne ResumeДокумент2 страницыEvans Shianne Resumeapi-490664291Оценок пока нет
- Construccion Barcaza PDFДокумент19 страницConstruccion Barcaza PDFMariano MarcosОценок пока нет
- Laporan - Pendahuluan PJK FixДокумент8 страницLaporan - Pendahuluan PJK FixNndaydnaОценок пока нет
- Dehydration PPДокумент17 страницDehydration PPApol PenОценок пока нет
- Pleural EffusionsДокумент41 страницаPleural Effusionssanjivdas100% (1)
- Noninvasive Ventilation Reduces Mortality in Severe PneumoniaДокумент4 страницыNoninvasive Ventilation Reduces Mortality in Severe PneumoniaMulyasari LindaОценок пока нет
- Cirugia ToraxДокумент117 страницCirugia ToraxErwin GuerreroОценок пока нет
- David CarsonДокумент24 страницыDavid CarsonanandnikОценок пока нет
- Sophie Griswold Recc Letter Mary OconnellДокумент1 страницаSophie Griswold Recc Letter Mary Oconnellapi-356127291Оценок пока нет
- Colistin Package Insert PDFДокумент2 страницыColistin Package Insert PDFRachelОценок пока нет
- HEYER VizOR 6 - Manual 1.0 EN PDFДокумент128 страницHEYER VizOR 6 - Manual 1.0 EN PDFkalandorka92Оценок пока нет
- MUSKULOSKELETAL Supplemental SlidesДокумент180 страницMUSKULOSKELETAL Supplemental Slidesstuffednurse100% (1)
- Mnemonic Devices for Medical EducationДокумент9 страницMnemonic Devices for Medical EducationJhey MalanyaonОценок пока нет
- NCP Epidural HemДокумент32 страницыNCP Epidural HemKatrina PonceОценок пока нет