Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Tpa ChecklistДокумент1 страницаTpa Checklistapi-269001337Оценок пока нет
- Case 23 Methadone ScriptДокумент1 страницаCase 23 Methadone Scriptapi-269001337Оценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Alteplase AlgorithmДокумент1 страницаAlteplase Algorithmapi-269001337Оценок пока нет
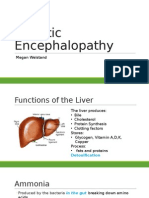
- Megan EncephalopathyДокумент19 страницMegan Encephalopathyapi-269001337Оценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Pechakucha Presentation - How To Prolong Life in Heart Failure For UploadДокумент20 страницPechakucha Presentation - How To Prolong Life in Heart Failure For Uploadapi-269001337Оценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Management of StemisДокумент20 страницManagement of Stemisapi-269001337Оценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
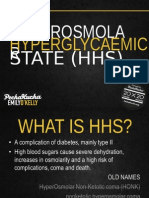
- Compressed Emilyokelly PetchkutchaДокумент20 страницCompressed Emilyokelly Petchkutchaapi-269001337Оценок пока нет
- Complications of DMДокумент19 страницComplications of DMapi-269001337Оценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
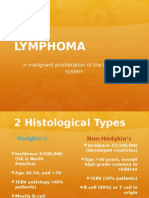
- Ed Pecha Kucha LymphomaДокумент20 страницEd Pecha Kucha Lymphomaapi-269001337Оценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Gropes - Tom SharpeДокумент73 страницыThe Gropes - Tom SharpeCrisMorillas100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- PT3 ELSA SampleДокумент8 страницPT3 ELSA Samplefattahjamal50% (2)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- English Assignment 1 The TrialДокумент4 страницыEnglish Assignment 1 The TrialAditi Pradhan0% (1)
- SCIOLY Div C Event Rules 2013-2014Документ31 страницаSCIOLY Div C Event Rules 2013-2014alexpark97Оценок пока нет
- MalariaДокумент4 страницыMalarianafrabОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Rethinking Food Security in Humanitarian Response: Paper Presented To The Food Security Forum, Rome, April 16 - 18, 2008Документ82 страницыRethinking Food Security in Humanitarian Response: Paper Presented To The Food Security Forum, Rome, April 16 - 18, 2008OxfamОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Insufficient Portable Water Threatens The Health and Development of The People in KibaweДокумент3 страницыInsufficient Portable Water Threatens The Health and Development of The People in KibaweDesiree Aranggo MangueraОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- SarvestianДокумент16 страницSarvestianMd50% (2)
- Arthritis Case Presentation - Dr. KlaesДокумент27 страницArthritis Case Presentation - Dr. KlaesShanti VennamОценок пока нет
- Daily Lesson Plan - NSTP1Документ3 страницыDaily Lesson Plan - NSTP1Charity Mae DoradoОценок пока нет
- Senate Hearing, 107TH Congress - Halting The Spread of Hiv/aids: Future Efforts in The U.S. Bilateral and Multilateral ResponseДокумент184 страницыSenate Hearing, 107TH Congress - Halting The Spread of Hiv/aids: Future Efforts in The U.S. Bilateral and Multilateral ResponseScribd Government DocsОценок пока нет
- 2011 Joint Commission Tissue StandardsДокумент24 страницы2011 Joint Commission Tissue StandardsPatient Safety MyОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Kode Icd XДокумент4 страницыKode Icd XAnonymous 3DxWnxОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Anti-HSV-2 IgG Herpes Simplex Virus Type 2Документ2 страницыAnti-HSV-2 IgG Herpes Simplex Virus Type 2ElenaОценок пока нет
- Fever With HemiplegiaДокумент65 страницFever With HemiplegiaMohit JainОценок пока нет
- Molecular Techniques For Detection, Species DifferentiationДокумент43 страницыMolecular Techniques For Detection, Species DifferentiationUziel Castillo VelazquezОценок пока нет
- Diseases of Lungs BLACKWOODДокумент360 страницDiseases of Lungs BLACKWOODG AnshuОценок пока нет
- Difteria Nigeria 2014Документ6 страницDifteria Nigeria 2014primaОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Abdulraheem Et AlДокумент10 страницAbdulraheem Et AlLaoye Abdulrahman AdewaleОценок пока нет
- PEPFAR Country Operational Plane (COP) Guidance 2010 Programs - June 29 2009 FinalДокумент147 страницPEPFAR Country Operational Plane (COP) Guidance 2010 Programs - June 29 2009 FinalAccessible Journal Media: Peace Corps DocumentsОценок пока нет
- Term Paper Tungkol Sa DengueДокумент5 страницTerm Paper Tungkol Sa Dengueaflsikxgf100% (1)
- Vestige Sharp Air PurifierДокумент6 страницVestige Sharp Air PurifierSamir K MishraОценок пока нет
- Brief Introduction To Protozoan Diseases of PoultryДокумент5 страницBrief Introduction To Protozoan Diseases of Poultrykarki Keadr Dr100% (4)
- BacteriaДокумент5 страницBacteriaShin RyuОценок пока нет
- Drug StudyДокумент3 страницыDrug Studymike_steven12Оценок пока нет
- Superficial and Cutaneous MycosesДокумент36 страницSuperficial and Cutaneous MycosesMich BagamanoОценок пока нет
- Infectious Diarrhoea: Laboratory Investigation ofДокумент36 страницInfectious Diarrhoea: Laboratory Investigation ofputra nisaОценок пока нет
- AcupressureДокумент3 страницыAcupressuregautamlipika100% (2)
- Protein Synthesis Inhibitors 2Документ25 страницProtein Synthesis Inhibitors 2AliImadAlKhasakiОценок пока нет
- Faith Script PDFДокумент1 страницаFaith Script PDFCamry Nicole CahimatОценок пока нет