Вам также может понравиться
- Assessment Nursing Diagnosis Planning Implementation OutcomeДокумент2 страницыAssessment Nursing Diagnosis Planning Implementation OutcomeBethel Ann Cordova100% (1)
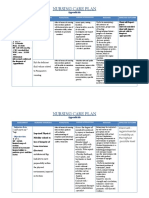
- Nursing Care PlanДокумент1 страницаNursing Care PlanErica Lagsa100% (1)
- NURSING CARE PLAN For Post Operative Cesarian SectionДокумент2 страницыNURSING CARE PLAN For Post Operative Cesarian SectionKaren Joyce Costales Magtanong100% (3)
- Nursing Care Plan For Cesarean SectionДокумент5 страницNursing Care Plan For Cesarean SectionJon Gab Paquit85% (33)
- Nursing Care Plan Cesarian DeliveryДокумент2 страницыNursing Care Plan Cesarian Deliveryderic97% (39)
- Nursing Care Plan (Acute Pain For Ceasarean Birth) HYPOTHETICALДокумент2 страницыNursing Care Plan (Acute Pain For Ceasarean Birth) HYPOTHETICALmarife84% (19)
- Nursing Care Plan Cesarean DeliveryДокумент2 страницыNursing Care Plan Cesarean DeliveryLei Ortega50% (4)
- Cesarian Section Case PresentationДокумент26 страницCesarian Section Case PresentationMae Azores86% (51)
- Postpartum CareДокумент9 страницPostpartum CareFreida Marie PiczonОценок пока нет
- Nursing Case Study C SectionДокумент12 страницNursing Case Study C SectionRiojane75% (8)
- Cs - Cesarean SectionДокумент19 страницCs - Cesarean Sectiondaph-me75% (16)
- NCP-Risk For InfectionДокумент4 страницыNCP-Risk For InfectionMarianne May Loquias100% (4)
- NCP On Postpartum MotherДокумент13 страницNCP On Postpartum MotherLenjun89% (57)
- Nursing Assessment and Interventions for Episiotomy Wound CareДокумент2 страницыNursing Assessment and Interventions for Episiotomy Wound Carenethcecilia90% (10)
- NCP: Labor Stage 1 Latent PhaseДокумент9 страницNCP: Labor Stage 1 Latent PhaseJavieОценок пока нет
- CS NCPДокумент3 страницыCS NCPAllan VillanuevaОценок пока нет
- Nursing Diagnosis Background Study Inference Goals and Objectives Interventions Rationale EvaluationДокумент5 страницNursing Diagnosis Background Study Inference Goals and Objectives Interventions Rationale EvaluationAubrey SungaОценок пока нет
- Postpartum Cesarean Section Case StudyДокумент17 страницPostpartum Cesarean Section Case StudyWeng Maesa MontemayorОценок пока нет
- Activity Intolerance DeliveryДокумент3 страницыActivity Intolerance Deliveryjunex123100% (2)
- All NCPsДокумент83 страницыAll NCPsDennis Nyambane Momanyi100% (6)
- Case Study On Breech BirthДокумент65 страницCase Study On Breech BirthSujan Shrestha94% (32)
- Cesarean SectionДокумент22 страницыCesarean SectionKarlo Bartolome100% (2)
- NCP - Impaired Skin IntegrityДокумент4 страницыNCP - Impaired Skin IntegrityColette Marie PerezОценок пока нет
- NCP For Caesarian Delivery (Breech Presentation)Документ2 страницыNCP For Caesarian Delivery (Breech Presentation)Raymond BasiloniaОценок пока нет
- Cesarean Section CaseStudyДокумент23 страницыCesarean Section CaseStudyDada Malicsi LandichoОценок пока нет
- Nursing Care Plan of The MotherДокумент20 страницNursing Care Plan of The Motherbuang2390% (382)
- Ovarian Cancer NCPДокумент7 страницOvarian Cancer NCPAsterlyn Coniendo100% (1)
- Risk For Infection Related To Presence of Surgical Wounds As Evidenced by MER 2nd DegreeДокумент3 страницыRisk For Infection Related To Presence of Surgical Wounds As Evidenced by MER 2nd DegreeSenyorita KHaye75% (12)
- Nursing Care PlanДокумент5 страницNursing Care Planseanamir100% (5)
- Nursing Interventions to Manage Postpartum Pain and Prevent ComplicationsДокумент6 страницNursing Interventions to Manage Postpartum Pain and Prevent ComplicationsAna LuisaОценок пока нет
- NCP Escaran.Документ3 страницыNCP Escaran.Roswell Almodiel EscaranОценок пока нет
- SP CSДокумент4 страницыSP CSKhan HansОценок пока нет
- Case Discussion: Mayan, Mercurio, Murillo BSN 2-AДокумент11 страницCase Discussion: Mayan, Mercurio, Murillo BSN 2-ADhen MarcОценок пока нет
- Nursing Process Care Plan Format: Patient Is A Non-SmokerДокумент2 страницыNursing Process Care Plan Format: Patient Is A Non-SmokerDavid PerezОценок пока нет
- NCP and Drug Study For Ob WardДокумент7 страницNCP and Drug Study For Ob WardAce Fabrigas100% (1)
- 2nd NCPДокумент4 страницы2nd NCPjoidaОценок пока нет
- Nursing Care PlanДокумент2 страницыNursing Care PlanMariel GamaloОценок пока нет
- Pain Related To Perineal Suture NCPДокумент3 страницыPain Related To Perineal Suture NCPDharylle CariñoОценок пока нет
- NCP Post Op (Impaired and Risk For Infection)Документ4 страницыNCP Post Op (Impaired and Risk For Infection)Carl J.Оценок пока нет
- NCP NSD 2Документ3 страницыNCP NSD 2Warren Bilog OleaОценок пока нет
- Copy of NCP Format)Документ4 страницыCopy of NCP Format)shai raОценок пока нет
- Clinical Portrait Pertinent DataДокумент9 страницClinical Portrait Pertinent DataGermin CesaОценок пока нет
- Acute PainДокумент4 страницыAcute PainIvan Jules P. PALMARESОценок пока нет
- NCP FamedДокумент1 страницаNCP FamedAbegail MierОценок пока нет
- NCP NSDДокумент3 страницыNCP NSDshigemasamayumi60% (5)
- Case Scenario - Nursing Care Plan (DR - Magsingal)Документ1 страницаCase Scenario - Nursing Care Plan (DR - Magsingal)Cristyl Shine BariaoОценок пока нет
- Nursing Care Plan: Assessment Nursing Diagnosis Rationale Planning Intervention S Rationale EvaluationДокумент7 страницNursing Care Plan: Assessment Nursing Diagnosis Rationale Planning Intervention S Rationale EvaluationNo EulОценок пока нет
- NCP Ectopic PregnancyДокумент2 страницыNCP Ectopic PregnancykatrinajhorelletillesОценок пока нет
- SAINT PAUL UNIVERSITY NURSING CARE PLAN FOR ACUTE PAINДокумент2 страницыSAINT PAUL UNIVERSITY NURSING CARE PLAN FOR ACUTE PAINJanice SolamilloОценок пока нет
- NCP 2Документ2 страницыNCP 2Loreily ShyreenОценок пока нет
- Nursing Care Plan for Acute Chest PainДокумент3 страницыNursing Care Plan for Acute Chest PainMelDred Cajes BolandoОценок пока нет
- NCP PainДокумент2 страницыNCP PainKimОценок пока нет
- Nursing Care PlanДокумент5 страницNursing Care PlankingpinОценок пока нет
- Nursing Care Plan: Acute PainДокумент4 страницыNursing Care Plan: Acute PainEvet VaxbmОценок пока нет
- Subjective Data: Objective Data: - Well Appearing But Independent Nursing Interventions: - Review Intraoperative Desired Outcome. Goal Met. Patient Was Able ToДокумент3 страницыSubjective Data: Objective Data: - Well Appearing But Independent Nursing Interventions: - Review Intraoperative Desired Outcome. Goal Met. Patient Was Able ToMariel GamaloОценок пока нет
- Cues Nursing Diagnosis Planning Nursing Interventions Rationale EvaluationДокумент3 страницыCues Nursing Diagnosis Planning Nursing Interventions Rationale EvaluationVie RahОценок пока нет
- Nursing-Care-Plan-J P VДокумент8 страницNursing-Care-Plan-J P VMa. Ferimi Gleam BajadoОценок пока нет
- Or NCPДокумент5 страницOr NCPjelopigar921Оценок пока нет
- Nursing Care Plan of Breech PresentationДокумент14 страницNursing Care Plan of Breech PresentationDr-Sanjay Singhania100% (3)
- NCP PostpartumДокумент6 страницNCP PostpartumLovely Anne ArqueroОценок пока нет
- Schwannoma L1-L2Документ4 страницыSchwannoma L1-L2Mae AzoresОценок пока нет
- ACLS Updated NotesДокумент2 страницыACLS Updated NotesMae AzoresОценок пока нет
- Acknowledgement and DedicationДокумент2 страницыAcknowledgement and DedicationMae AzoresОценок пока нет
- Sleep Disorders EditedДокумент9 страницSleep Disorders EditedMae AzoresОценок пока нет
- Physical Assessment For Patient With DM Type1Документ4 страницыPhysical Assessment For Patient With DM Type1Mae AzoresОценок пока нет
- Document Tcap-Draft ALSДокумент77 страницDocument Tcap-Draft ALSMae AzoresОценок пока нет
- Focus-Nursing Care Plan For Sleep DisordersДокумент9 страницFocus-Nursing Care Plan For Sleep DisordersMae AzoresОценок пока нет
- Dengue FeverДокумент5 страницDengue FeverMae AzoresОценок пока нет
- Nursing Care Plan Cues Nursing Diagnosis Objectives Nursing Intervention Rationale EvaluationДокумент6 страницNursing Care Plan Cues Nursing Diagnosis Objectives Nursing Intervention Rationale EvaluationMae AzoresОценок пока нет
- Sexually Connotative Disorders - ScribdДокумент18 страницSexually Connotative Disorders - ScribdMae AzoresОценок пока нет
- Syphillis CDN FinalДокумент13 страницSyphillis CDN FinalMae AzoresОценок пока нет
- CDN AmoebiasisДокумент3 страницыCDN AmoebiasisMae AzoresОценок пока нет
- The Learning Experience of A Student Nurse, A Critical AnalysisДокумент7 страницThe Learning Experience of A Student Nurse, A Critical AnalysisMae Azores100% (2)
- Status AsthmaticusДокумент6 страницStatus AsthmaticusMae Azores100% (1)
- Developing Work Groups For Community Health DevelopmentДокумент7 страницDeveloping Work Groups For Community Health DevelopmentMae Azores100% (1)
- Cesarian Section Case PresentationДокумент26 страницCesarian Section Case PresentationMae Azores86% (51)
- An Open Hand Amidst of SunsetsДокумент5 страницAn Open Hand Amidst of SunsetsMae AzoresОценок пока нет
- Yale Insulin Drip Protocol (Target 100 139) PDFДокумент2 страницыYale Insulin Drip Protocol (Target 100 139) PDFAprilia Christi SiwiОценок пока нет
- Thopaz InstructivoДокумент54 страницыThopaz InstructivomichelRamirezОценок пока нет
- Quality Risk Management ImplementationДокумент38 страницQuality Risk Management ImplementationAbdul NasirОценок пока нет
- Avoiding Blood Gases Errors Handbook PDFДокумент20 страницAvoiding Blood Gases Errors Handbook PDFkinnusaraiОценок пока нет
- Paediatric Anesthesiology - Anesthesiology ClinicsДокумент309 страницPaediatric Anesthesiology - Anesthesiology ClinicsAbdullah QaziОценок пока нет
- Nasal TraumaДокумент5 страницNasal TraumaRae Marie AquinoОценок пока нет
- Jurnal Case Report Carcinoma Maxillaris PDFДокумент3 страницыJurnal Case Report Carcinoma Maxillaris PDFEnvhy WinaОценок пока нет
- Pycnogenol For Cardiovascular Health - V2010Документ12 страницPycnogenol For Cardiovascular Health - V2010LubimOffОценок пока нет
- Nursing Ethics: Raymund Christopher R. Dela Peña, RN, RMДокумент23 страницыNursing Ethics: Raymund Christopher R. Dela Peña, RN, RMrnrmmanphd100% (1)
- Seminar 5 - Thyroid Disease in PregnancyДокумент25 страницSeminar 5 - Thyroid Disease in PregnancyHakimah K. SuhaimiОценок пока нет
- Rituxan RituximabДокумент21 страницаRituxan RituximabMavisОценок пока нет
- ACLS Manual Provider 2016Документ207 страницACLS Manual Provider 2016AhmedShareef100% (9)
- CT venography reliability vs DSAДокумент7 страницCT venography reliability vs DSAwan hanisaОценок пока нет
- Apollo Hospitals - First-World Health Care at Emerging - Market PricesДокумент3 страницыApollo Hospitals - First-World Health Care at Emerging - Market PricesNaveen Chander Dhar100% (1)
- Ibogaine Treatment NotesДокумент4 страницыIbogaine Treatment NotesjesterstableОценок пока нет
- Pre - and Post Test Cardiac ArrhythmiasДокумент6 страницPre - and Post Test Cardiac ArrhythmiasEköw Santiago JavierОценок пока нет
- PERSONALITY DISORDERS: CLUSTERS A AND BДокумент58 страницPERSONALITY DISORDERS: CLUSTERS A AND BJoanneMontalboОценок пока нет
- Prolonged Paroxysmal Sympathetic Storming Associated With Spontaneous Subarachnoid HemorrhageДокумент5 страницProlonged Paroxysmal Sympathetic Storming Associated With Spontaneous Subarachnoid Hemorrhageiri_balОценок пока нет
- Medicine TT - Yr5-Batch 7 Rot-1, Gp-1Документ10 страницMedicine TT - Yr5-Batch 7 Rot-1, Gp-1Priya GKОценок пока нет
- Summary of Product Characteristics: 4.1 Therapeutic IndicationsДокумент6 страницSummary of Product Characteristics: 4.1 Therapeutic IndicationsMustika Dwi SusilowatiОценок пока нет
- 300 Video Lectures About Narcissists and PsychopathsДокумент20 страниц300 Video Lectures About Narcissists and PsychopathsSam VakninОценок пока нет
- Psychiatric Medication Guidelines Pregnancy LactationДокумент27 страницPsychiatric Medication Guidelines Pregnancy LactationSunija SelvamОценок пока нет
- Lois - Pemicu 5Документ143 страницыLois - Pemicu 5anggita tri lestariОценок пока нет
- Drug Study and NCPДокумент9 страницDrug Study and NCPDan Dan ManaoisОценок пока нет
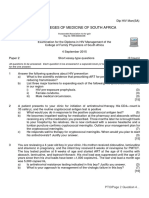
- Dip HIV Man (SA) Past Papers - 2015 2nd Semester 24-1-2017Документ2 страницыDip HIV Man (SA) Past Papers - 2015 2nd Semester 24-1-2017matentenОценок пока нет
- Hawaii Medical PediatricsДокумент10 страницHawaii Medical PediatricstinkictijoОценок пока нет
- What Is First Aid? A Simple: Definition 1Документ3 страницыWhat Is First Aid? A Simple: Definition 1Robert D.PalbanОценок пока нет
- Hemorrhagic StrokeДокумент30 страницHemorrhagic StrokeAstrina SupandyОценок пока нет
- Medical CertificateДокумент126 страницMedical CertificateAnonymous mummYD0% (1)
- 110 TOP SURGERY Multiple Choice Questions and Answers PDF - Medical Multiple Choice Questions PDFДокумент11 страниц110 TOP SURGERY Multiple Choice Questions and Answers PDF - Medical Multiple Choice Questions PDFaziz0% (1)