Вам также может понравиться
- Employee Coaching Form: Insert Company Name Insert LogoДокумент1 страницаEmployee Coaching Form: Insert Company Name Insert LogoBADBOYОценок пока нет
- Authorization To DeductДокумент1 страницаAuthorization To Deductumanichole25Оценок пока нет
- Annual Leave RecordДокумент1 страницаAnnual Leave RecordAshok DadasОценок пока нет
- Overtime TimesheetДокумент1 страницаOvertime TimesheetDawn EganОценок пока нет
- Caterpillar Equipment Training Solutions Operator Training Program Registration FormДокумент2 страницыCaterpillar Equipment Training Solutions Operator Training Program Registration FormpercyОценок пока нет
- Form Exit Interview HgsДокумент2 страницыForm Exit Interview HgsRusdiana RiyandaОценок пока нет
- Job Order Performa: For Engineering Dept' Use OnlyДокумент2 страницыJob Order Performa: For Engineering Dept' Use OnlysohailОценок пока нет
- Employee CoachingДокумент1 страницаEmployee CoachingShara Mayola PedranzaОценок пока нет
- Application For Salary AdvanceДокумент1 страницаApplication For Salary AdvanceAhefaz Shaikh100% (1)
- Daftar Absensi HarianДокумент1 страницаDaftar Absensi HarianVeren MonettaОценок пока нет
- Clearance Form Revised - Apr (1) - 30Документ2 страницыClearance Form Revised - Apr (1) - 30Gabriel Dave AlamoОценок пока нет
- PGR02 - Changing of SupervisorДокумент4 страницыPGR02 - Changing of SupervisorKAVITHA A/P PARIMAL MoeОценок пока нет
- Authorization To Deduct 2Документ1 страницаAuthorization To Deduct 2umanichole25Оценок пока нет
- Interest Free LoanДокумент1 страницаInterest Free Loanmuhammad.zubairbcsОценок пока нет
- Compensatory/Overtime Request Form (Non-Exempt Employees Only)Документ1 страницаCompensatory/Overtime Request Form (Non-Exempt Employees Only)Sunny MarientesОценок пока нет
- Contract Labor AgreementДокумент1 страницаContract Labor AgreementRAIEL COLARDOОценок пока нет
- Department of Business Administration Intern Evaluation FormДокумент1 страницаDepartment of Business Administration Intern Evaluation FormSazidul Islam PrantikОценок пока нет
- Short Leave Form: Employee's Signature Supervisor SignatureДокумент1 страницаShort Leave Form: Employee's Signature Supervisor SignaturesaeedОценок пока нет
- Monthly Safety Meeting MinutesДокумент2 страницыMonthly Safety Meeting Minuteswashi1349Оценок пока нет
- Annual Leave FormДокумент2 страницыAnnual Leave FormShafiq AtranОценок пока нет
- Construction Daily TimesheetДокумент1 страницаConstruction Daily Timesheetanilkumaranoop74Оценок пока нет
- Authority To Deduct FormДокумент1 страницаAuthority To Deduct FormLoise ValdezОценок пока нет
- Job Safety Analysis Form: InstructionsДокумент1 страницаJob Safety Analysis Form: InstructionsTamara Astri NirwanaОценок пока нет
- Clearance Form UpdatedДокумент1 страницаClearance Form UpdatedmarkanthonymailigОценок пока нет
- Professional Regulation Commission Cpe Council For Nursing: Republic of The PhilippinesДокумент1 страницаProfessional Regulation Commission Cpe Council For Nursing: Republic of The Philippinescraig garwynОценок пока нет
- C Off Form Rev00Документ1 страницаC Off Form Rev00Pradyuman Verma100% (2)
- Nomination of Supervisor FormДокумент3 страницыNomination of Supervisor FormMuhamad Kharizal bin AdzemyОценок пока нет
- Department of Business AdministrationДокумент1 страницаDepartment of Business AdministrationS.m. Sagor AhmmedОценок пока нет
- 1 CESS ABPT Project Nomination of SupervisorДокумент4 страницы1 CESS ABPT Project Nomination of SupervisorElyssa SatimanОценок пока нет
- PGR01 - Nomination of Supervisor - MasterДокумент2 страницыPGR01 - Nomination of Supervisor - MasterMuhammad Fakhrul Najmi JaafarОценок пока нет
- New Itinerary 2022Документ3 страницыNew Itinerary 2022Jeramae GabatoОценок пока нет
- Date DAY Time-In Time-OUT Total Hours Supervisor'S SignatureДокумент1 страницаDate DAY Time-In Time-OUT Total Hours Supervisor'S SignatureabbyОценок пока нет
- HR FRM 015 Greviance FormДокумент3 страницыHR FRM 015 Greviance FormAnna EgwimОценок пока нет
- Aep Clearance FormДокумент1 страницаAep Clearance FormGenelyn Mutya RevecheОценок пока нет
- CESB Resolution No. 1136Документ22 страницыCESB Resolution No. 1136rbulalakawОценок пока нет
- FormsДокумент6 страницFormsapi-279353598Оценок пока нет
- Orientation Checklist: Department OIC Employee's SignatureДокумент2 страницыOrientation Checklist: Department OIC Employee's Signaturechan_punchmeeОценок пока нет
- Actionplan TemplateДокумент2 страницыActionplan TemplateMoinuddin AnsariОценок пока нет
- Actionplan TemplateДокумент2 страницыActionplan TemplateDanaCecariОценок пока нет
- S T A P F: Your Logo Here Template Pyramid Model Tate EAM Ction Lanning ORMДокумент2 страницыS T A P F: Your Logo Here Template Pyramid Model Tate EAM Ction Lanning ORMKhad BakarОценок пока нет
- Actionplan TemplateДокумент2 страницыActionplan TemplateMaria LisaОценок пока нет
- Actionplan TemplateДокумент2 страницыActionplan TemplateMaria LisaОценок пока нет
- Actionplan TemplateДокумент2 страницыActionplan TemplateMaria LisaОценок пока нет
- Actionplan TemplateДокумент2 страницыActionplan Templatemallickss97Оценок пока нет
- HKSF Instructor Claim FormДокумент1 страницаHKSF Instructor Claim Formraymond tsangОценок пока нет
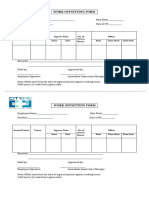
- Offsetting FormДокумент1 страницаOffsetting FormEdhilyn HurryОценок пока нет
- Application For EmploymentДокумент2 страницыApplication For EmploymentJessica Yirnaldy Rodriguez JimenezОценок пока нет
- Time Off Request FormДокумент1 страницаTime Off Request FormHRM ServicesОценок пока нет
- Future First Job Seeker Registration FormДокумент3 страницыFuture First Job Seeker Registration FormJonathan GillespieОценок пока нет
- N44 Ts Fuis 9 C 6Документ2 страницыN44 Ts Fuis 9 C 6weijeeОценок пока нет
- Maintenance RequestДокумент2 страницыMaintenance Requestsajid waqasОценок пока нет
- CPL FormДокумент1 страницаCPL FormElectrical jobОценок пока нет
- Daily Time RecordДокумент1 страницаDaily Time RecordChes TerОценок пока нет
- Work Completion CertificateДокумент1 страницаWork Completion CertificateDIVEETH MPОценок пока нет
- Sample Parts FormДокумент2 страницыSample Parts FormallenОценок пока нет
- Emergency Loan Form 2018Документ1 страницаEmergency Loan Form 2018Jansen TanОценок пока нет
- Employee Write-Up Form With Improvement PlanДокумент2 страницыEmployee Write-Up Form With Improvement PlanfrankОценок пока нет
- Leave ApplicationДокумент1 страницаLeave ApplicationFaraz Anwar AbroОценок пока нет
- Hacking for Beginners: Comprehensive Guide on Hacking Websites, Smartphones, Wireless Networks, Conducting Social Engineering, Performing a Penetration Test, and Securing Your Network (2022)От EverandHacking for Beginners: Comprehensive Guide on Hacking Websites, Smartphones, Wireless Networks, Conducting Social Engineering, Performing a Penetration Test, and Securing Your Network (2022)Оценок пока нет