Вам также может понравиться
- Susan Edwards - Neurological PhysiotherapyДокумент293 страницыSusan Edwards - Neurological Physiotherapyharcaian_cristina90% (20)
- Physiotherapy in Neuro Conditions Glady Samuel Raj PDFДокумент331 страницаPhysiotherapy in Neuro Conditions Glady Samuel Raj PDFAnkita Tiwari82% (50)
- Orthopaedic Management in Cerebral Palsy, 2nd EditionОт EverandOrthopaedic Management in Cerebral Palsy, 2nd EditionHelen Meeks HorstmannРейтинг: 3 из 5 звезд3/5 (2)
- Opening A Private Practice in Occupational Therapy: Earn .1 Aota CeuДокумент9 страницOpening A Private Practice in Occupational Therapy: Earn .1 Aota CeuRey John MonjeОценок пока нет
- AOPA Handout NewParadigms Sciences IMPДокумент34 страницыAOPA Handout NewParadigms Sciences IMPAnup PednekarОценок пока нет
- Angelman Syndrome - Identification and ManagementДокумент10 страницAngelman Syndrome - Identification and ManagementFajar YuniftiadiОценок пока нет
- Dyssemia Rating ScaleДокумент8 страницDyssemia Rating ScaleHazardous7Оценок пока нет
- 2 Introduction To TheoryДокумент14 страниц2 Introduction To TheoryNurul Izzah Wahidul AzamОценок пока нет
- The Bobath Concept - A Model To Illustrate Clinical PracticeДокумент14 страницThe Bobath Concept - A Model To Illustrate Clinical PracticeCynthia Arriagada Olavarria100% (1)
- Myotonometer ManualДокумент30 страницMyotonometer ManualRucsandra Avirvarei100% (1)
- Mobilization and Stimulation of Neuromuscular Tissue (MaSoNT)От EverandMobilization and Stimulation of Neuromuscular Tissue (MaSoNT)Оценок пока нет
- Facilitation For A CP ChildДокумент4 страницыFacilitation For A CP ChildpraveenОценок пока нет
- Application of Facilitatory Approaches in Developmental DysarthriaДокумент22 страницыApplication of Facilitatory Approaches in Developmental Dysarthriakeihoina keihoinaОценок пока нет
- ApproachДокумент37 страницApproachAshu AshОценок пока нет
- Home Base Intervention OtДокумент9 страницHome Base Intervention OtPaulinaОценок пока нет
- Minimal Brain Dysfunction in ChildrenДокумент31 страницаMinimal Brain Dysfunction in ChildrenDAVIDBROS64Оценок пока нет
- Orthopedic Manual Therapy Chadcook3rdPTMASUDДокумент30 страницOrthopedic Manual Therapy Chadcook3rdPTMASUDHisham Al ShamiОценок пока нет
- 2015 TimpДокумент2 страницы2015 TimpCdiat San ClementeОценок пока нет
- The Bobath Concept inДокумент12 страницThe Bobath Concept inCedricFernandezОценок пока нет
- Bobath Therapy and Hemiplegia - HemiHelp PDFДокумент22 страницыBobath Therapy and Hemiplegia - HemiHelp PDFLall JingerppangОценок пока нет
- Cerebral Palsy Road Map:: What To Expect As Your Child GrowsДокумент40 страницCerebral Palsy Road Map:: What To Expect As Your Child GrowsSergio Curtean100% (1)
- Activity Analysis, Creativity and Playfulness in Pediatric Occupational TherapyДокумент16 страницActivity Analysis, Creativity and Playfulness in Pediatric Occupational TherapySofia VieiraОценок пока нет
- DR Luh - Role of PMR in NICUДокумент50 страницDR Luh - Role of PMR in NICUad putraОценок пока нет
- Hip Displacement in Cerebral PalsyДокумент9 страницHip Displacement in Cerebral PalsyJohannesSchoppmannОценок пока нет
- Part One: and Practical Aspects of TestingДокумент22 страницыPart One: and Practical Aspects of TestingCIK FATHINОценок пока нет
- Torticollis and Your BabyДокумент14 страницTorticollis and Your BabySham ObaidatОценок пока нет
- PHYSIOTIMES Vol.7, Issue 5, March'2016Документ1 страницаPHYSIOTIMES Vol.7, Issue 5, March'2016PHYSIOTIMESОценок пока нет
- Mcimt NDT Kids at 1Документ12 страницMcimt NDT Kids at 1api-485106673Оценок пока нет
- Rehab of Patients With HemiplegiaДокумент2 страницыRehab of Patients With HemiplegiaMilijana D. DelevićОценок пока нет
- Langerhans-Cell Histiocytosis: Review ArticleДокумент13 страницLangerhans-Cell Histiocytosis: Review ArticleHanifah ArroziОценок пока нет
- Mirror Therapy PDFДокумент26 страницMirror Therapy PDFrusu_alexandra_4Оценок пока нет
- Pediatric Therapy Program: Cayuga Medical Center at IthacaДокумент2 страницыPediatric Therapy Program: Cayuga Medical Center at IthacaMhmd IrakyОценок пока нет
- Rib Cage CoursesДокумент11 страницRib Cage CoursesPBОценок пока нет
- Cerebral Palsy Info SheetДокумент3 страницыCerebral Palsy Info Sheetapi-263996400100% (1)
- My Child Without Limits - Cerebral PalsyДокумент46 страницMy Child Without Limits - Cerebral PalsyBernard Owusu100% (1)
- Physical Therapy Management of Congenital Muscular.2Документ47 страницPhysical Therapy Management of Congenital Muscular.2Physio EbookОценок пока нет
- Help Patients Manage Equinus DeformityДокумент5 страницHelp Patients Manage Equinus DeformityRodrigo HightowerОценок пока нет
- Stretching With Children With Cerebral Palsy What.8 PDFДокумент6 страницStretching With Children With Cerebral Palsy What.8 PDFNurul FadhillahОценок пока нет
- Baby Treatment Based On NDT Principles Baby Treatment Based On NDT PrinciplesДокумент2 страницыBaby Treatment Based On NDT Principles Baby Treatment Based On NDT PrinciplesHiten J Thakker0% (1)
- Physiotherapy Assessment and Treatment On PICUДокумент54 страницыPhysiotherapy Assessment and Treatment On PICUBatool Rehman100% (2)
- Instrumental Activities Daily Living: Try ThisДокумент11 страницInstrumental Activities Daily Living: Try ThisbalryoОценок пока нет
- Occupational Therapy Rehabilitation Paraplegic PatientДокумент7 страницOccupational Therapy Rehabilitation Paraplegic PatientAlina PasăreОценок пока нет
- Shoulder Impingement GuidelinesДокумент3 страницыShoulder Impingement GuidelinesTasha MillerОценок пока нет
- Pyramid & Extrapyramidal DisordersДокумент5 страницPyramid & Extrapyramidal Disordersjoelh9Оценок пока нет
- Neurological Assessment in the First Two Years of LifeОт EverandNeurological Assessment in the First Two Years of LifeGiovanni CioniОценок пока нет
- Gait in Children With Cerebral PalsyДокумент5 страницGait in Children With Cerebral PalsyvarahamihirОценок пока нет
- PANat - Thetrical - Air Splints - Talas Pneumaticas Margaret JohnstoneДокумент44 страницыPANat - Thetrical - Air Splints - Talas Pneumaticas Margaret JohnstonePedro GouveiaОценок пока нет
- What Is Ot PedsДокумент2 страницыWhat Is Ot Pedsapi-232349586Оценок пока нет
- Satco Clinical WorkbookДокумент6 страницSatco Clinical WorkbookKidz to Adultz Exhibitions100% (1)
- Lateral Epicondylitis - Tennis Ellbow HandoutДокумент5 страницLateral Epicondylitis - Tennis Ellbow Handoutgermany23Оценок пока нет
- Einspieler Etal JPsychol 2008Документ7 страницEinspieler Etal JPsychol 2008ramopavelОценок пока нет
- DyslexiaДокумент19 страницDyslexiaJubie MathewОценок пока нет
- The Importance of TouchДокумент5 страницThe Importance of TouchJavier Estrada CampayoОценок пока нет
- GMFMДокумент1 страницаGMFMFlorin Dragos Caprita100% (1)
- Essence of The Bobath Concept in The Treatment of Children With PCДокумент14 страницEssence of The Bobath Concept in The Treatment of Children With PCCéline FrédérickОценок пока нет
- Gait AnalysisДокумент49 страницGait AnalysisKrishna KumariОценок пока нет
- Guidelines Motor Disorders Assessment and InterventionДокумент322 страницыGuidelines Motor Disorders Assessment and InterventionWilhelm HeinleinОценок пока нет
- Relationship Between Hip, Knee and AnkleДокумент47 страницRelationship Between Hip, Knee and AnkleshivnairОценок пока нет
- PD 8278 Energy Conservation PDFДокумент4 страницыPD 8278 Energy Conservation PDFahmad kusnaeniОценок пока нет
- Cerebral Palsy Care Giving GuideДокумент511 страницCerebral Palsy Care Giving GuideJoel OntiverosОценок пока нет
- Instructor's Manual: Catherine Meriano, JD, MHS, OTR/LДокумент10 страницInstructor's Manual: Catherine Meriano, JD, MHS, OTR/LDaNelle McPhaddenОценок пока нет
- Cerebral Palsy: Signs and CausesДокумент2 страницыCerebral Palsy: Signs and CausesAhmad Rais DahyarОценок пока нет
- Physiotherapy Based On The Bobath ConceptpdfДокумент6 страницPhysiotherapy Based On The Bobath ConceptpdfmatsОценок пока нет
- Diagnostics I - PulsesДокумент15 страницDiagnostics I - Pulsesg23164100% (1)
- Advised Rest and If Required Low Intensity Light Activities During The Period of T/T of 10-12 DaysДокумент2 страницыAdvised Rest and If Required Low Intensity Light Activities During The Period of T/T of 10-12 Daysdrprasant100% (1)
- Presenting: (Diclofenac Diethylamine B.P. 100 MG)Документ2 страницыPresenting: (Diclofenac Diethylamine B.P. 100 MG)drprasantОценок пока нет
- Clinic Theater 2 - Class 5Документ2 страницыClinic Theater 2 - Class 5drprasant100% (1)
- Clinic Theater 2 - Class 4Документ2 страницыClinic Theater 2 - Class 4drprasantОценок пока нет
- Presenting: (Ketoprofen I.P. 20 MG)Документ2 страницыPresenting: (Ketoprofen I.P. 20 MG)drprasantОценок пока нет
- Capri Institute of Manual Therapy: Address For Correspondence: - A-64, Hans Apartment, East Arjun Nagar, CBDДокумент1 страницаCapri Institute of Manual Therapy: Address For Correspondence: - A-64, Hans Apartment, East Arjun Nagar, CBDdrprasantОценок пока нет
- Given The Code in The Exhibit What Is The Result? A. B. C. D. Answer: B Explanation: ZДокумент1 страницаGiven The Code in The Exhibit What Is The Result? A. B. C. D. Answer: B Explanation: ZdrprasantОценок пока нет
- Ebook NPTE TipsДокумент11 страницEbook NPTE Tipsdrprasant100% (1)
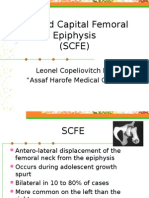
- Slipped Capital Femoral EpiphysisДокумент12 страницSlipped Capital Femoral EpiphysisdrprasantОценок пока нет
- Disorders of LobesДокумент55 страницDisorders of LobesdrprasantОценок пока нет
- PNF and Other TechniquesДокумент8 страницPNF and Other TechniquesdrprasantОценок пока нет
- Manipulation Therapy For Tennis Elbow:-: Prasant Gupta BPT Final YearДокумент2 страницыManipulation Therapy For Tennis Elbow:-: Prasant Gupta BPT Final YeardrprasantОценок пока нет
- Neural Mobilizations (By David Butler) : How To Stretch A Nerve???Документ1 страницаNeural Mobilizations (By David Butler) : How To Stretch A Nerve???drprasantОценок пока нет
- KiblerДокумент10 страницKiblerdrprasantОценок пока нет
- Pediatrictone Management: Sathya Vadivelu,, Anne Stratton,, Wendy PierceДокумент10 страницPediatrictone Management: Sathya Vadivelu,, Anne Stratton,, Wendy PierceDeborah SalinasОценок пока нет
- Neurologic Examination of The Newborn - UpToDateДокумент40 страницNeurologic Examination of The Newborn - UpToDateAMIT TYAGIОценок пока нет
- Neurological Rehabilitation - Spasticity and Contractures in Clinical Practice and Research PDFДокумент312 страницNeurological Rehabilitation - Spasticity and Contractures in Clinical Practice and Research PDFioabv100% (1)
- Muscle Energy Technique: Concepts & MethodsДокумент24 страницыMuscle Energy Technique: Concepts & MethodssandipandassarmaОценок пока нет
- Effectiveness of Serial Casting in Patients With Severe Cerebral Spasticity: A Comparison StudyДокумент7 страницEffectiveness of Serial Casting in Patients With Severe Cerebral Spasticity: A Comparison StudyDaniel MarvasoОценок пока нет
- Mayston People With Cerebral Palsy Effects of and Perspectives For TherapyДокумент20 страницMayston People With Cerebral Palsy Effects of and Perspectives For TherapyΒασίλης ΒασιλείουОценок пока нет
- Examination of The Child With CerebralpalsyДокумент52 страницыExamination of The Child With CerebralpalsyRiaz KhanОценок пока нет
- Clinical Evaluation and Management of Spasticity PDFДокумент397 страницClinical Evaluation and Management of Spasticity PDFRicardo Pedro100% (1)
- Eddy Anderson, The Founder of Rebound Therapy, Answers The Question: What Is Rebound Therapy?Документ4 страницыEddy Anderson, The Founder of Rebound Therapy, Answers The Question: What Is Rebound Therapy?aaronjdriver2248Оценок пока нет
- Cerebral Palsy Practice Essentials: Signs and SymptomsДокумент11 страницCerebral Palsy Practice Essentials: Signs and SymptomsTahsinur RahmanОценок пока нет
- Bobath ConceptДокумент5 страницBobath ConceptdrprasantОценок пока нет
- MiorelДокумент1 страницаMiorelApostolos T.Оценок пока нет
- Normal Tone & Abnormal Tone - Handling TechniquesДокумент2 страницыNormal Tone & Abnormal Tone - Handling TechniquesWasemBhatОценок пока нет
- Neuro LabДокумент37 страницNeuro LabIonut SegaОценок пока нет
- Graham 2016Документ25 страницGraham 2016Constanzza Arellano LeivaОценок пока нет
- Paratonia in Dementia A Systematic ReviewДокумент23 страницыParatonia in Dementia A Systematic ReviewResidentes PsiquiatríaОценок пока нет
- Gen - Sug. 2Документ32 страницыGen - Sug. 2Mahir RathodОценок пока нет
- Thesis Rma FinalllllДокумент25 страницThesis Rma FinallllljoanaОценок пока нет
- Training To Optimize Performance Driving Reorganization?: Exercise and Functional in Stroke: NeuralДокумент10 страницTraining To Optimize Performance Driving Reorganization?: Exercise and Functional in Stroke: NeuralPhooi Yee LauОценок пока нет
- Coma Recovery Scale - Revised (CRS-R) PDFДокумент16 страницComa Recovery Scale - Revised (CRS-R) PDFLeli MulyatiОценок пока нет
- 02 Padure, L. Spastic Hip in Cerebral PalsyДокумент4 страницы02 Padure, L. Spastic Hip in Cerebral PalsyminichoixОценок пока нет
- Neurological PhysiotherapyДокумент252 страницыNeurological PhysiotherapyZrakaSunca93% (14)
- Remediating Motor ControlДокумент66 страницRemediating Motor Controlhis.thunder122100% (3)
- Spastic ParaplegiaДокумент7 страницSpastic ParaplegiaDio ResnaОценок пока нет
- Module 17 Building and Enhancing New Literacies Across The Curriculum BADARANДокумент10 страницModule 17 Building and Enhancing New Literacies Across The Curriculum BADARANLance AustriaОценок пока нет
- Upper & Lower Limb ExaminationДокумент20 страницUpper & Lower Limb Examinationcvmqx7yppd100% (1)
- JAAOS - Volume 11 - Issue 05 September & October 2003Документ83 страницыJAAOS - Volume 11 - Issue 05 September & October 2003kenthepaОценок пока нет