Вам также может понравиться
- QuestДокумент1 страницаQuestRho Vince Caño MalagueñoОценок пока нет
- TonsillectomyДокумент27 страницTonsillectomyRho Vince Caño MalagueñoОценок пока нет
- ASTHMA TreatmentДокумент27 страницASTHMA TreatmentRho Vince Caño Malagueño0% (1)
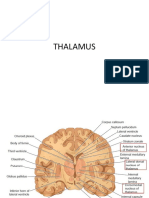
- ThalamusДокумент30 страницThalamusRho Vince Caño Malagueño100% (1)
- Operating Room StandardsДокумент28 страницOperating Room StandardsRho Vince Caño MalagueñoОценок пока нет
- Cranial Epidural AbscessДокумент31 страницаCranial Epidural AbscessRho Vince Caño MalagueñoОценок пока нет
- The Bradyarrhythmias: Disorders of The Atrioventricular NodeДокумент34 страницыThe Bradyarrhythmias: Disorders of The Atrioventricular NodeRho Vince Caño MalagueñoОценок пока нет
- CD-NTG BupcДокумент9 страницCD-NTG BupcRho Vince Caño MalagueñoОценок пока нет
- Cabinet: Title NameДокумент5 страницCabinet: Title NameRho Vince Caño MalagueñoОценок пока нет
- Reading As A Physiological ProcessДокумент2 страницыReading As A Physiological ProcessRho Vince Caño Malagueño89% (9)
- Arrowroot Powder vs. Cornstarch: Why Arrowroot Powder Is A Better ChoiceДокумент53 страницыArrowroot Powder vs. Cornstarch: Why Arrowroot Powder Is A Better ChoiceRho Vince Caño MalagueñoОценок пока нет
- LABOR and Delivery: Cristina Cleofe, RM BSN - IiiДокумент17 страницLABOR and Delivery: Cristina Cleofe, RM BSN - IiiRho Vince Caño MalagueñoОценок пока нет
- Arrow of GodДокумент24 страницыArrow of GodRho Vince Caño Malagueño100% (1)
- Pediatric Sample ExamДокумент5 страницPediatric Sample ExamRho Vince Caño MalagueñoОценок пока нет
- A Typology of Nursing Problems in Family Nursing ProblemДокумент5 страницA Typology of Nursing Problems in Family Nursing ProblemRho Vince Caño MalagueñoОценок пока нет
- QuestionnaireДокумент4 страницыQuestionnaireRho Vince Caño MalagueñoОценок пока нет
- MYASTHENIA GRAVIS Case PresentationДокумент78 страницMYASTHENIA GRAVIS Case PresentationRho Vince Caño Malagueño50% (4)
- Henry Sy Success StoryДокумент6 страницHenry Sy Success StoryRho Vince Caño MalagueñoОценок пока нет
- Transmittal Letter or Cover Letter-1Документ3 страницыTransmittal Letter or Cover Letter-1Rho Vince Caño MalagueñoОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Development of The Urinary Organs (3rd - 4th Week)Документ16 страницDevelopment of The Urinary Organs (3rd - 4th Week)ridhaОценок пока нет
- Assignment 1 - InfertilityДокумент41 страницаAssignment 1 - InfertilityRenu Ravina ChandОценок пока нет
- Word List UrinalysisДокумент2 страницыWord List Urinalysischerry100% (1)
- Human Sexuality Unit: Reproductive SystemsДокумент38 страницHuman Sexuality Unit: Reproductive SystemsMary Grace CacalОценок пока нет
- Summer 2122 Aubf Lab Periodical Test 2Документ38 страницSummer 2122 Aubf Lab Periodical Test 2RuchieОценок пока нет
- Imaging in Genitourinary SystemДокумент36 страницImaging in Genitourinary SystemAlkaustariyah LubisОценок пока нет
- Urine Formation Steps Filtration: Dr. Sumaiya KhanДокумент4 страницыUrine Formation Steps Filtration: Dr. Sumaiya KhanZeleen Ann SaberonОценок пока нет
- Benign Prostatic Hyperplasia (BPH) : Ahmad AbdulraheemДокумент35 страницBenign Prostatic Hyperplasia (BPH) : Ahmad AbdulraheemAhmad AltarefeОценок пока нет
- Class 4 - Circulatory and Excretory System Questions and AnswersДокумент4 страницыClass 4 - Circulatory and Excretory System Questions and Answersanil guptaОценок пока нет
- Biology Form 5 - The Human Urinary SystemДокумент50 страницBiology Form 5 - The Human Urinary Systemilykhairunnisa0% (1)
- URO Final 2023Документ31 страницаURO Final 2023دشيرين إبراهيمОценок пока нет
- ME Sci 10 Q3 1001 PSДокумент17 страницME Sci 10 Q3 1001 PSsino56601Оценок пока нет
- Fantiyao Reproductive System Group 2Документ4 страницыFantiyao Reproductive System Group 2Jushelle Anne Tigoy PilareОценок пока нет
- Male Reproductive Teacher NotesДокумент3 страницыMale Reproductive Teacher Notespaigebotlon30Оценок пока нет
- APAPU Scientific ProgrammeДокумент13 страницAPAPU Scientific ProgrammeFarooque SohooОценок пока нет
- Techno India Groip Public School, Balurghat MCQ: SESSION 2019 - 2020 Class - Xi Sub - Biology Full Marks - TimeДокумент3 страницыTechno India Groip Public School, Balurghat MCQ: SESSION 2019 - 2020 Class - Xi Sub - Biology Full Marks - Timekoushik kunduОценок пока нет
- RENAL WORKSHEET Anatomy AnswerДокумент10 страницRENAL WORKSHEET Anatomy AnswerJohnny eawОценок пока нет
- Bladder DiverticulaДокумент23 страницыBladder DiverticulaJeanette CallejasОценок пока нет
- Presentation On - Clinical Implication of Female ReproductiveДокумент13 страницPresentation On - Clinical Implication of Female ReproductiveMahenurОценок пока нет
- Renal QuizДокумент5 страницRenal Quiztyno MajonОценок пока нет
- Unit No: Topic:: 2 Human Reproduction Review of Anatomy and Physiology of Human Reproductive System: Male and FemaleДокумент31 страницаUnit No: Topic:: 2 Human Reproduction Review of Anatomy and Physiology of Human Reproductive System: Male and FemaleSavita HanamsagarОценок пока нет
- Diagnostic Management URINALYSISДокумент3 страницыDiagnostic Management URINALYSISjhappo31Оценок пока нет
- Nur 194 Mod 2Документ5 страницNur 194 Mod 2Mendoza Winchelle Kyla R.Оценок пока нет
- Semen Collection, Evaluation and Processing IДокумент23 страницыSemen Collection, Evaluation and Processing IKristi Smith0% (1)
- Introduction To Semen AnalysisДокумент13 страницIntroduction To Semen AnalysisShaye Toliao GeligОценок пока нет
- Lab 8-Urinary System Anatomy and UrinalysisДокумент17 страницLab 8-Urinary System Anatomy and UrinalysisAeriara GraysonОценок пока нет
- Retractile TestisДокумент7 страницRetractile TestisAhmad Rahmat Ramadhan TantuОценок пока нет
- S9 - End-Of-Unit 4 TestДокумент3 страницыS9 - End-Of-Unit 4 Testpranavi jagarlamudi100% (2)
- NettersДокумент32 страницыNettersYogi SetiawanОценок пока нет
- Human Growth and Development: 5th Grade FemaleДокумент28 страницHuman Growth and Development: 5th Grade FemalemarigenОценок пока нет