Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
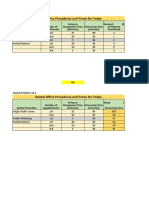
- Dental Office Procedures and Times For TodayДокумент3 страницыDental Office Procedures and Times For TodayCleofe Mae Piñero AseñasОценок пока нет
- Post Insertion Denture ProblemsДокумент48 страницPost Insertion Denture ProblemsAswitha GanapathyОценок пока нет
- Managing Second MolarsДокумент5 страницManaging Second MolarsEvelin CastilloОценок пока нет
- History of ProsthodonticsДокумент121 страницаHistory of ProsthodonticsArthi Ramalingam aОценок пока нет
- Endo Perio ProblemsДокумент8 страницEndo Perio ProblemsSarah KahilОценок пока нет
- Pulpectomy & ApexificationДокумент72 страницыPulpectomy & ApexificationSimrah AjmalОценок пока нет
- Class Ii Amalgam Restorations: Occlusal Outline Form (Occlusal Step)Документ4 страницыClass Ii Amalgam Restorations: Occlusal Outline Form (Occlusal Step)Depressed CowОценок пока нет
- A Longitudinal Study of Combined Periodontal and Prosthetic Treatment of Patients With Advanced Periodontal DiseaseДокумент7 страницA Longitudinal Study of Combined Periodontal and Prosthetic Treatment of Patients With Advanced Periodontal DiseaseLedir Luciana Henley de AndradeОценок пока нет
- Integrated Esthetics in Periodontics and ImplantologyДокумент818 страницIntegrated Esthetics in Periodontics and ImplantologyOmar Villamizar100% (1)
- DEvelopment of Normal OcclusionДокумент7 страницDEvelopment of Normal OcclusionMohammed HassanОценок пока нет
- 7 Prevention of Periodontal DiseaseДокумент58 страниц7 Prevention of Periodontal DiseaseYoussef ElbeharyОценок пока нет
- Workflow Description of Additively Manufactured Clear Silicone Indexes For Injected Provisional Restorations: A Novel TechniqueДокумент9 страницWorkflow Description of Additively Manufactured Clear Silicone Indexes For Injected Provisional Restorations: A Novel Techniquedrzana78Оценок пока нет
- Clasificacion Fisuras LPHДокумент72 страницыClasificacion Fisuras LPHkarenОценок пока нет
- Journal 012010 PDFДокумент76 страницJournal 012010 PDFAlysonОценок пока нет
- Quality Assessment of Systematic Reviews On Alveolar Socket Preservation.Документ9 страницQuality Assessment of Systematic Reviews On Alveolar Socket Preservation.andreita_loppОценок пока нет
- Mouth and OropharynxДокумент17 страницMouth and OropharynxNursidar Pascual MukattilОценок пока нет
- How To Save Your TeethДокумент193 страницыHow To Save Your TeethTanon Jaturonnatee100% (2)
- Occlusal Registration in Removable Partial DentureДокумент70 страницOcclusal Registration in Removable Partial DentureHassan BotaniОценок пока нет
- Two-Implant-Supported Mandibular Overdentures: Do Clinical Denture Quality and Inter-Implant Distance Affect Patient Satisfaction?Документ7 страницTwo-Implant-Supported Mandibular Overdentures: Do Clinical Denture Quality and Inter-Implant Distance Affect Patient Satisfaction?Ahmad FadhilОценок пока нет
- DR - Shaheen Part 2 PDFДокумент13 страницDR - Shaheen Part 2 PDFmidhunОценок пока нет
- Mandibular 2 PremolarДокумент63 страницыMandibular 2 PremolarDr.O.R.GANESAMURTHIОценок пока нет
- Biologic Width Evaluation and Correction of Its ViДокумент7 страницBiologic Width Evaluation and Correction of Its Visari elyОценок пока нет
- 1) The Teeth That Are Used For Cracking Hard Food AreДокумент6 страниц1) The Teeth That Are Used For Cracking Hard Food Arechhavi bhatnagarОценок пока нет
- Mini SKY Prospekt 2017 009911GBДокумент2 страницыMini SKY Prospekt 2017 009911GBLucian Catalin CalinОценок пока нет
- Scope of Practice: General Dental CouncilДокумент11 страницScope of Practice: General Dental CouncilAlexandra LauraОценок пока нет
- Chemical Burn 4Документ2 страницыChemical Burn 4Yeni PuspitasariОценок пока нет
- Ethics of DentistryДокумент20 страницEthics of DentistrytayabakhanОценок пока нет
- Ohi Case StudyДокумент11 страницOhi Case Studyapi-308499727100% (1)
- Module 6: Radiographic Techniques: Lesson 16: Periapical Radiographs & Intraoral SurveysДокумент101 страницаModule 6: Radiographic Techniques: Lesson 16: Periapical Radiographs & Intraoral SurveysSai Krishna YellapuОценок пока нет
- Steco Catalogue-05 15Документ74 страницыSteco Catalogue-05 15topobuccia100% (1)