Вам также может понравиться
- Complete Guide To ECGДокумент78 страницComplete Guide To ECGAnas YahyaОценок пока нет
- Pharmacovigilance DefinationsДокумент32 страницыPharmacovigilance DefinationsKadir AmirОценок пока нет
- Pharma Reviewer From VinnyДокумент16 страницPharma Reviewer From VinnyKris TejereroОценок пока нет
- Rectal Bleeding OverviewДокумент7 страницRectal Bleeding OverviewYanceHanzieОценок пока нет
- Acute Incisional Hernia: Theme From September 2011 ExamДокумент146 страницAcute Incisional Hernia: Theme From September 2011 ExamVimal Kumar YadavОценок пока нет
- Nursing Guide Urinary Catheterization ProcedureДокумент6 страницNursing Guide Urinary Catheterization ProcedureDencel BarramedaОценок пока нет
- 01 - Signs and Symptoms of Git DisordersДокумент51 страница01 - Signs and Symptoms of Git DisordersRere AnugrahОценок пока нет
- Acute Pain Abdomen in Surgical PracticeДокумент34 страницыAcute Pain Abdomen in Surgical PracticedrakashnardeОценок пока нет
- NCM 104 Cellular Aberration Lecture 2007Документ104 страницыNCM 104 Cellular Aberration Lecture 2007Kris TejereroОценок пока нет
- Valvular Heart Disease To TW FinalДокумент13 страницValvular Heart Disease To TW FinalMohammed ElSayedОценок пока нет
- AppendectomyДокумент8 страницAppendectomyDark AghanimОценок пока нет
- Liver Cirrhosis Case PresДокумент77 страницLiver Cirrhosis Case Presmarlx580% (5)
- IV Fluid Types and UsesДокумент6 страницIV Fluid Types and UsesKiara Denise TamayoОценок пока нет
- Basic Examination of BloodДокумент48 страницBasic Examination of BloodmedinoОценок пока нет
- Acute Abdominal Pain GuideДокумент77 страницAcute Abdominal Pain GuideGraceline Margaretha Marsintauly SianiparОценок пока нет
- Comman Sign and SymptomsДокумент3 страницыComman Sign and SymptomsSachin SinghОценок пока нет
- Urinary System DisordersДокумент120 страницUrinary System DisordersFaith Levi Alecha Alferez100% (1)
- Hemiplegia Rehabilitation TechniquesДокумент11 страницHemiplegia Rehabilitation TechniquesFares EL DeenОценок пока нет
- Cardiovascular Diagnostic Tests & Procedures.Документ25 страницCardiovascular Diagnostic Tests & Procedures.Salman KhanОценок пока нет
- Dietary Guidelines For Indians-NINДокумент138 страницDietary Guidelines For Indians-NINsaradhi26Оценок пока нет
- Appendicitis 130421042532 Phpapp02Документ32 страницыAppendicitis 130421042532 Phpapp02Rabie'ahBahananОценок пока нет
- Urinary EliminationДокумент101 страницаUrinary EliminationJade Giordano100% (1)
- Resistant Hypertension. AHAДокумент38 страницResistant Hypertension. AHAEderEmmanuelMartinezRuiz100% (1)
- Coronary Artery Disease and HypertensionДокумент8 страницCoronary Artery Disease and HypertensionsnehaОценок пока нет
- Abdominal AssessmentДокумент11 страницAbdominal Assessmentasa100% (1)
- WHO MDR 2020 Handbook Treatment PDFДокумент88 страницWHO MDR 2020 Handbook Treatment PDFYuanita GunawanОценок пока нет
- Nursing Leadership and Management Prelims Lesson 1-5Документ4 страницыNursing Leadership and Management Prelims Lesson 1-5Paul Christian P. Santos, RN100% (14)
- Emergency DrugsДокумент17 страницEmergency Drugsapi-3853350100% (12)
- Physical Assessment FormДокумент5 страницPhysical Assessment FormJam AustinОценок пока нет
- Cowperitis Remedy Characteristics Symptoms Patient Worse by Patient Better by A State of Fear Anxiety Anguish of Mind and BodyДокумент5 страницCowperitis Remedy Characteristics Symptoms Patient Worse by Patient Better by A State of Fear Anxiety Anguish of Mind and Bodymadhavkrishna gargОценок пока нет
- Chest Examination New SsДокумент16 страницChest Examination New SsNAIОценок пока нет
- Physical Assessment ResultДокумент4 страницыPhysical Assessment Resultariskendell15Оценок пока нет
- CatheterizationДокумент31 страницаCatheterizationAlfi Nur Hanifah100% (1)
- Pulmonary Embolism Guide: Causes, Symptoms & DiagnosisДокумент60 страницPulmonary Embolism Guide: Causes, Symptoms & DiagnosisRafika RaraОценок пока нет
- Inguinal Hernias and Abdominal Wall Defects: Murad Nuserat & Abd AL-Rahman AlhelwДокумент51 страницаInguinal Hernias and Abdominal Wall Defects: Murad Nuserat & Abd AL-Rahman AlhelwRashed ShatnawiОценок пока нет
- Viral Exanthem (Main)Документ94 страницыViral Exanthem (Main)Starlet Rhonadez Bito-onon OrielОценок пока нет
- PATIENT 1 Nursing Assessment FormДокумент5 страницPATIENT 1 Nursing Assessment FormndemboloveОценок пока нет
- Uroflowmetry: A Guide to Urine Flow StudiesДокумент41 страницаUroflowmetry: A Guide to Urine Flow StudiesSri HariОценок пока нет
- Acquired Heart DiseasesДокумент41 страницаAcquired Heart DiseasesSaman SarKoОценок пока нет
- Topic 5 Nursing Care of The High-Risk Post-Partal ClientsДокумент51 страницаTopic 5 Nursing Care of The High-Risk Post-Partal ClientsMarissa A AquinoОценок пока нет
- GIT Examination - Clinical Skills With DRДокумент8 страницGIT Examination - Clinical Skills With DRNaveen KovalОценок пока нет
- What Causes Urinary Retention?Документ4 страницыWhat Causes Urinary Retention?darkz_andreaslimОценок пока нет
- Community Health Nursing ReviewerДокумент11 страницCommunity Health Nursing Revieweroxidalaj88% (24)
- Angelito L. Ramos Jr. RN Clinical InstructorДокумент68 страницAngelito L. Ramos Jr. RN Clinical Instructorraymondblade18100% (17)
- Nursing Care Plan Risk For Urinary RetentionДокумент4 страницыNursing Care Plan Risk For Urinary RetentionReginald Julia100% (2)
- Test Report Gupta DiagnosisДокумент17 страницTest Report Gupta Diagnosisdrblgupta1973100% (1)
- Hemorrhoids: 1. Chief ComplaintДокумент4 страницыHemorrhoids: 1. Chief Complaintdrnareshkumar3281Оценок пока нет
- Drug Name Mechanism of Action Indication Side Effects Nursing Responsibilities Generic Name: Occasional: DuringДокумент2 страницыDrug Name Mechanism of Action Indication Side Effects Nursing Responsibilities Generic Name: Occasional: Duringhahaha100% (1)
- Common Dental ProblemsДокумент14 страницCommon Dental ProblemsInternational Journal of Innovative Science and Research TechnologyОценок пока нет
- What's New in Respiratory DisordersДокумент4 страницыWhat's New in Respiratory DisorderssobanОценок пока нет
- Ragay - Notes of EentДокумент15 страницRagay - Notes of Eentaynin39Оценок пока нет
- Different Diagnostic Procedure of Typhoid Fever AДокумент8 страницDifferent Diagnostic Procedure of Typhoid Fever AdjebrutОценок пока нет
- Eye Path12Документ45 страницEye Path12JillKellyОценок пока нет
- Widal Agglutination Test PDFДокумент5 страницWidal Agglutination Test PDFशशांक तिवारीОценок пока нет
- PBL PgamboaДокумент6 страницPBL PgamboaLeanne Princess GamboaОценок пока нет
- Anorectal DiseasesДокумент15 страницAnorectal DiseaseserickОценок пока нет
- Nursing Process 3Документ10 страницNursing Process 3Shubhra Sheoran100% (1)
- Abdominal Aortic AneurysmДокумент2 страницыAbdominal Aortic AneurysmAria MontgomeryОценок пока нет
- Portal hypertension diagnosis and managementДокумент23 страницыPortal hypertension diagnosis and managementSumathi Gopinath100% (1)
- Atom EcgДокумент7 страницAtom Ecgsutan IskandarsyahОценок пока нет
- The 5 Most Common Sports InjuriesДокумент4 страницыThe 5 Most Common Sports InjuriesAngeline SahagunОценок пока нет
- Supracondylar FractureДокумент53 страницыSupracondylar Fracturedesire kbpОценок пока нет
- Cardiotonic DrugsДокумент67 страницCardiotonic DrugsLady Mae Ramos100% (1)
- Angina PectorisДокумент17 страницAngina PectorisRacel HernandezОценок пока нет
- Glossitis Symptoms, Causes and TreatmentДокумент10 страницGlossitis Symptoms, Causes and Treatmentfarida ulfa100% (1)
- 322 Copd Writing AssignmentДокумент5 страниц322 Copd Writing Assignmentapi-353335798Оценок пока нет
- 14) PPT ROMAN Salah Training - StudentsДокумент342 страницы14) PPT ROMAN Salah Training - Studentsamer sohailОценок пока нет
- Clinical Examination of A Diabetic Patient ErДокумент38 страницClinical Examination of A Diabetic Patient Erlxnalexander100% (1)
- Acute Pancreatitis NOTESДокумент17 страницAcute Pancreatitis NOTESsameeha semiОценок пока нет
- Case Presentation: by Michael ArmstrongДокумент21 страницаCase Presentation: by Michael ArmstrongWirawan Amirul BahriОценок пока нет
- Basic Examination of BloodДокумент6 страницBasic Examination of BloodMadeleinePriscillaОценок пока нет
- 46-Year-Old Man With Abnormal Lipid ProfileДокумент3 страницы46-Year-Old Man With Abnormal Lipid ProfileCamiiliita Fernández La TorreОценок пока нет
- Anemia 130809044630 Phpapp01Документ21 страницаAnemia 130809044630 Phpapp01Siddharth Das100% (1)
- Problem-based Approach to Gastroenterology and HepatologyОт EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisОценок пока нет
- A Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsОт EverandA Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsОценок пока нет
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsОт EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsОценок пока нет
- PCM (8) Test For Significance (Dr. Tante)Документ151 страницаPCM (8) Test For Significance (Dr. Tante)Kris TejereroОценок пока нет
- Anatomy Lab IdentificationДокумент3 страницыAnatomy Lab IdentificationKris TejereroОценок пока нет
- MechanicsДокумент10 страницMechanicsKris TejereroОценок пока нет
- ABC AccomodationДокумент55 страницABC AccomodationKris TejereroОценок пока нет
- Ronel NaireДокумент4 страницыRonel NaireKris TejereroОценок пока нет
- Of The Main Characters in The PlagueДокумент2 страницыOf The Main Characters in The PlagueKris TejereroОценок пока нет
- Anatomy Lab IdentificationДокумент6 страницAnatomy Lab IdentificationKris TejereroОценок пока нет
- Histology RespiДокумент4 страницыHistology RespiKris TejereroОценок пока нет
- Germany DE: State of Health in The EUДокумент24 страницыGermany DE: State of Health in The EUKris TejereroОценок пока нет
- Physics Formulas for Pressure, Water Pressure, and TrigonometryДокумент2 страницыPhysics Formulas for Pressure, Water Pressure, and TrigonometryKris TejereroОценок пока нет
- MechanicsДокумент10 страницMechanicsKris TejereroОценок пока нет
- MechanicsДокумент10 страницMechanicsKris TejereroОценок пока нет
- Of The Main Characters in The PlagueДокумент2 страницыOf The Main Characters in The PlagueKris TejereroОценок пока нет
- School Stage RoofingДокумент12 страницSchool Stage RoofingKris TejereroОценок пока нет
- By: Kris Lyn L. TejereoДокумент30 страницBy: Kris Lyn L. TejereoKris TejereroОценок пока нет
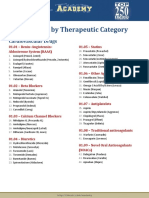
- Drug List by Therapeutic Category: Cardiovascular DrugsДокумент7 страницDrug List by Therapeutic Category: Cardiovascular DrugsAloah122346Оценок пока нет
- Backbone Drug StudyДокумент1 страницаBackbone Drug StudyKris TejereroОценок пока нет
- Cellular AberrationДокумент71 страницаCellular AberrationKris TejereroОценок пока нет
- HematologyДокумент10 страницHematologyKris TejereroОценок пока нет
- Level of CompetencyДокумент7 страницLevel of CompetencyKris TejereroОценок пока нет
- Contoh Soal Uji Kompetensi Keperawatan KomunitasДокумент39 страницContoh Soal Uji Kompetensi Keperawatan KomunitasUmairohSetengahTiga67% (3)
- Vaccine Minimum Age at 1st Dose Number of Doses Dose Minimum Interval Between Doses Route Site ReasonДокумент4 страницыVaccine Minimum Age at 1st Dose Number of Doses Dose Minimum Interval Between Doses Route Site ReasonKris TejereroОценок пока нет
- Area Inspection Palpation Auscultation Percussion: Physical AssessmentДокумент6 страницArea Inspection Palpation Auscultation Percussion: Physical AssessmentKris TejereroОценок пока нет
- Postobstructive Diuresis: Clinical ReviewДокумент6 страницPostobstructive Diuresis: Clinical ReviewRara Aulia IIОценок пока нет
- Tubes, Catheters, and DrainsДокумент17 страницTubes, Catheters, and DrainsInnocent BachiОценок пока нет
- NURSING CARE PLAN - Impaired Urinary EliminationДокумент2 страницыNURSING CARE PLAN - Impaired Urinary EliminationDaniel Andre S. SomorayОценок пока нет
- Xatral XL treats enlarged prostateДокумент6 страницXatral XL treats enlarged prostateasdwasdОценок пока нет
- Acute Bacterial Prostatitis: Diagnosis and ManagementДокумент7 страницAcute Bacterial Prostatitis: Diagnosis and ManagementMilla MartinsОценок пока нет
- Abstract in EnglishДокумент1 страницаAbstract in EnglishKhoirun FitriaОценок пока нет
- Urinary IncontinenceДокумент7 страницUrinary IncontinenceasuratosОценок пока нет
- Signs of Urethral TraumaДокумент6 страницSigns of Urethral TraumaWenna Grace OdtujanОценок пока нет
- Urinary Catheterization: By: Michael John Z. Principio, RN, RM, MancДокумент22 страницыUrinary Catheterization: By: Michael John Z. Principio, RN, RM, MancSarahlaine BrazasОценок пока нет
- Urological Symptomatology in Patients With Reflex Sympathetic DystrophyДокумент8 страницUrological Symptomatology in Patients With Reflex Sympathetic DystrophyMihaela LitovcencoОценок пока нет
- AnuriaДокумент4 страницыAnuriachoobiОценок пока нет
- Benign Prostatic Hyperplasia - StatPearls - NCBI BookshelfДокумент26 страницBenign Prostatic Hyperplasia - StatPearls - NCBI Bookshelfantonio.mastrangelo.999Оценок пока нет
- Peran Dokter Keluarga Dalam Penatalaksanaan Komprehensif Keganasan Prostat 2018 DR Yusuf Alam R PDFДокумент87 страницPeran Dokter Keluarga Dalam Penatalaksanaan Komprehensif Keganasan Prostat 2018 DR Yusuf Alam R PDFBestariayuОценок пока нет
- Urinary System DisordersДокумент14 страницUrinary System DisordersGideon P. CasasОценок пока нет
- Safety and Pain-Relief Efficacy of Urethral Catheter With Local-Anesthetic Injection PortДокумент5 страницSafety and Pain-Relief Efficacy of Urethral Catheter With Local-Anesthetic Injection PortYudhi AuliaОценок пока нет
- Case Presentation On NutritionДокумент15 страницCase Presentation On NutritionDyvi DuranteОценок пока нет
- PROSTATITISДокумент25 страницPROSTATITISRoppeОценок пока нет
- Urinary CatheterizationДокумент3 страницыUrinary CatheterizationElla LobenariaОценок пока нет
- BPH PresentationДокумент33 страницыBPH PresentationKwabena AmankwaОценок пока нет
- FON Mcqs From Nurses Lab Web by Abdullah Danish, Educational PlatformДокумент1 096 страницFON Mcqs From Nurses Lab Web by Abdullah Danish, Educational PlatformShayan ShayanОценок пока нет
- MS Urology Program CurriculumДокумент73 страницыMS Urology Program CurriculumZeeshan AliОценок пока нет