Вам также может понравиться
- Psychology, Psychiatry and Chronic PainОт EverandPsychology, Psychiatry and Chronic PainStephen P. TyrerОценок пока нет
- Zofran (Ondansetron)Документ3 страницыZofran (Ondansetron)EОценок пока нет
- Zocor (Simvastin)Документ3 страницыZocor (Simvastin)Adrianne BazoОценок пока нет
- Chennai ThesisДокумент22 страницыChennai ThesisShradhanjali PandaОценок пока нет
- ZocorДокумент3 страницыZocorEОценок пока нет
- Gangguan TiroidДокумент37 страницGangguan Tiroidjung hoseokОценок пока нет
- Theragran (Multiple Vitamins)Документ3 страницыTheragran (Multiple Vitamins)EОценок пока нет
- Theragran (Multiple Vitamins)Документ3 страницыTheragran (Multiple Vitamins)Adrianne BazoОценок пока нет
- Classification, Epidemiology, Pathophysiology of HypertensionДокумент35 страницClassification, Epidemiology, Pathophysiology of Hypertensionastrid abrahamsОценок пока нет
- Reglan Drug CardДокумент4 страницыReglan Drug CardAdrianne BazoОценок пока нет
- DilaudidДокумент5 страницDilaudidE100% (2)
- International Gastroenterology Congress - ESG Talk 2022Документ65 страницInternational Gastroenterology Congress - ESG Talk 2022afroz01Оценок пока нет
- Hubungan Antara Peningkatan Kadar Tetraiodothyonine Dengan Asam Urat Pada Penderita Penyakit Graves Di Rumah Sakit Dr. Pirngadi MedaN tAHUN 2017Документ8 страницHubungan Antara Peningkatan Kadar Tetraiodothyonine Dengan Asam Urat Pada Penderita Penyakit Graves Di Rumah Sakit Dr. Pirngadi MedaN tAHUN 2017deprosa br gintingОценок пока нет
- Antidepressants and Mood Stabilisers: Professor DR Hussain Habil Professor and HOD Psychiatry MahsaДокумент23 страницыAntidepressants and Mood Stabilisers: Professor DR Hussain Habil Professor and HOD Psychiatry MahsaPATHMAPRIYA GANESANОценок пока нет
- Fulminant Hepatic Failure and Liver TransplantationДокумент104 страницыFulminant Hepatic Failure and Liver TransplantationtasarimkutusuОценок пока нет
- SSC 2012 Guidelines Teaching Glucose ControlДокумент19 страницSSC 2012 Guidelines Teaching Glucose ControlRaymark SalongaОценок пока нет
- Tylenol 500 MGДокумент3 страницыTylenol 500 MGEОценок пока нет
- NPS MedicineWise Thyroid Testing Algorithm v3Документ1 страницаNPS MedicineWise Thyroid Testing Algorithm v3Mikhael JHОценок пока нет
- TAP BlockДокумент27 страницTAP BlockSneha PanditОценок пока нет
- NURS 2516 Clinical Medications WorksheetsДокумент5 страницNURS 2516 Clinical Medications WorksheetsEОценок пока нет
- Biology of Estrogen & Progesterone Receptors: Benita S. KatzenellenbogenДокумент35 страницBiology of Estrogen & Progesterone Receptors: Benita S. KatzenellenbogenRiver GoldenОценок пока нет
- All About Thyroid 2019Документ45 страницAll About Thyroid 2019Octo IndradjajaОценок пока нет
- Tylenol Acetaminophen)Документ3 страницыTylenol Acetaminophen)EОценок пока нет
- Post Menopausal Osteoporosis: Evolution of Eu GuidanceДокумент27 страницPost Menopausal Osteoporosis: Evolution of Eu GuidanceNimal EshwarОценок пока нет
- Merck Sales by Product Category (1995-1997) IN ($ MILLION)Документ4 страницыMerck Sales by Product Category (1995-1997) IN ($ MILLION)aayushi bhandariОценок пока нет
- Lacerated Wound Forms (Artillo)Документ9 страницLacerated Wound Forms (Artillo)Al TheóОценок пока нет
- Opioid Toxicity: Nathaniel Katz, MD Harvard Medical School Boston, MAДокумент26 страницOpioid Toxicity: Nathaniel Katz, MD Harvard Medical School Boston, MAYohanes FirmansyahОценок пока нет
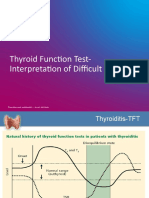
- TFT Interpretation of Difficult CasesДокумент51 страницаTFT Interpretation of Difficult CasesAditya GautamОценок пока нет
- DUTCH Results ExplainedДокумент9 страницDUTCH Results ExplainedFiona QuoiОценок пока нет
- Seizures/Epilepsy: Case PersentationДокумент14 страницSeizures/Epilepsy: Case PersentationAbdulmalik AliОценок пока нет
- Eletriptan - bsn2-C - Belen, Jessa MaeДокумент2 страницыEletriptan - bsn2-C - Belen, Jessa MaeJessa Mae BelenОценок пока нет
- Randomized Placebo-Controlled Trial of Adjuvant Therapy With Withania Somnifera in Parkinson'S Disease. (Wis-Pd)Документ25 страницRandomized Placebo-Controlled Trial of Adjuvant Therapy With Withania Somnifera in Parkinson'S Disease. (Wis-Pd)M Fahad SaleemОценок пока нет
- DR - Thitiya - New Pragmatic Treatment in HER2+ PatientsДокумент37 страницDR - Thitiya - New Pragmatic Treatment in HER2+ Patientst_t2822Оценок пока нет
- Research Article Review: Julianne M Barredo Dr. Victoria FischerДокумент10 страницResearch Article Review: Julianne M Barredo Dr. Victoria Fischerapi-639582054Оценок пока нет
- Research Based Paper UniversityДокумент2 страницыResearch Based Paper UniversitySimran SGОценок пока нет
- Prezentare Caz PsihiatrieДокумент25 страницPrezentare Caz PsihiatrieIrina NițulescuОценок пока нет
- Kuliah 10 Antitiroid 2014Документ32 страницыKuliah 10 Antitiroid 2014cccccОценок пока нет
- TSH Reagent Kit: B7P480 G71292R02Документ6 страницTSH Reagent Kit: B7P480 G71292R02Галина МиловановаОценок пока нет
- Call To See Patient PDFДокумент111 страницCall To See Patient PDFKevin KhawОценок пока нет
- Hypertensión Ese - Spin - Brochure - Rev. - 03 - LowДокумент12 страницHypertensión Ese - Spin - Brochure - Rev. - 03 - LowVICTOR losanОценок пока нет
- Pioneer Nursing College, Vadodara Master Rotation Plan For M.SC Nursing First YearДокумент2 страницыPioneer Nursing College, Vadodara Master Rotation Plan For M.SC Nursing First YearKinjal VasavaОценок пока нет
- Shared Decision Making Case StudyДокумент40 страницShared Decision Making Case StudylokeshОценок пока нет
- Al-Zaytoonah Private University of Jordan: Psychiatric Nursing DepartmentДокумент29 страницAl-Zaytoonah Private University of Jordan: Psychiatric Nursing DepartmentHeba_Al_KhozaeОценок пока нет
- Clinical Trial of Homoeopathic Preparations of Amyleum Nitrosum, Azathioprine Cocainum Muriaticum and Cyclosporine in HIV DiseaseДокумент34 страницыClinical Trial of Homoeopathic Preparations of Amyleum Nitrosum, Azathioprine Cocainum Muriaticum and Cyclosporine in HIV DiseaseDr Dushyant Kamal DhariОценок пока нет
- Stimulating - Loving - Caring - Integrated Psycosocial SupportДокумент1 страницаStimulating - Loving - Caring - Integrated Psycosocial SupportVickha Dian HapsariОценок пока нет
- Shugar1952 PDFДокумент8 страницShugar1952 PDFmikeОценок пока нет
- Treatment Options For PTSDДокумент8 страницTreatment Options For PTSDrapton56Оценок пока нет
- Estimulacion Craneal CES - Ray - SmithДокумент30 страницEstimulacion Craneal CES - Ray - Smithgonzalez1Оценок пока нет
- Danzi 2013Документ7 страницDanzi 2013Ana CortezОценок пока нет
- Update in Clinical Psychopharmacology: Peter A. Demaria, JR., M.D., FasamДокумент52 страницыUpdate in Clinical Psychopharmacology: Peter A. Demaria, JR., M.D., FasamZubair Mahmood KamalОценок пока нет
- Targeted Therapies in Renal Cell CarcinomaДокумент24 страницыTargeted Therapies in Renal Cell CarcinomabiomathenОценок пока нет
- 02 Lecture 10 Anti-Thyroid Drugs (DR Thatcher Pod Pharm 2022)Документ36 страниц02 Lecture 10 Anti-Thyroid Drugs (DR Thatcher Pod Pharm 2022)sahilaminОценок пока нет
- Dummy Client RAADS-R 2024-04-09Документ7 страницDummy Client RAADS-R 2024-04-09ciliogsmer56Оценок пока нет
- CCR3 6 1684Документ5 страницCCR3 6 1684FathkaHanifAbimanyuОценок пока нет
- Zocor (Simvastatin)Документ3 страницыZocor (Simvastatin)E100% (1)
- StorvasДокумент1 страницаStorvasShariq NishatОценок пока нет
- Infant Radiant Warmer: Service Manual GuideДокумент46 страницInfant Radiant Warmer: Service Manual GuideHemric50% (2)
- Cardiologia - EletrocardiografiaДокумент40 страницCardiologia - EletrocardiografiaDANIEL ALEJANDROОценок пока нет
- Anatomia - Diagnostica (PPTshare)Документ70 страницAnatomia - Diagnostica (PPTshare)DANIEL ALEJANDRO100% (1)
- Sindrome Del Corazon RotoДокумент6 страницSindrome Del Corazon RotoDANIEL ALEJANDROОценок пока нет
- 1.1 Trauma RaquimedularДокумент55 страниц1.1 Trauma RaquimedularDANIEL ALEJANDROОценок пока нет
- Cardiologia - EletrocardiografiaДокумент40 страницCardiologia - EletrocardiografiaDANIEL ALEJANDROОценок пока нет
- GertsmanДокумент6 страницGertsmandantevalerОценок пока нет
- Preprint Not Peer ReviewedДокумент9 страницPreprint Not Peer ReviewedpatrickОценок пока нет
- Chronic Fatigue SyndromeДокумент3 страницыChronic Fatigue Syndromereinfabz13Оценок пока нет
- Long COVID Major Findings Mechanisms Recommendations-2023Документ14 страницLong COVID Major Findings Mechanisms Recommendations-2023Zezinho zéОценок пока нет
- Summary of Recent Significant Findings in ME-CFS Research - Updated February 2019 PDFДокумент21 страницаSummary of Recent Significant Findings in ME-CFS Research - Updated February 2019 PDFEmilie ChateletОценок пока нет
- Fibromyalgia & Chronic FatigueДокумент4 страницыFibromyalgia & Chronic FatigueKarl JacobsОценок пока нет
- 4 Popular Myths and Misconceptions About Being An EmpathДокумент4 страницы4 Popular Myths and Misconceptions About Being An EmpathDragoș L. I. TeodorescuОценок пока нет
- VISION Loughton Edition 35 April 21Документ39 страницVISION Loughton Edition 35 April 21VISION PublicationsОценок пока нет
- Disclosure Log 2296Документ3 страницыDisclosure Log 2296api-257817850Оценок пока нет
- UntitledДокумент46 страницUntitledapi-257817850Оценок пока нет
- DR Sebi Herb ListДокумент2 страницыDR Sebi Herb ListJohn Rumatora100% (1)
- ACE Personal Trainer Manual Chapter 13Документ59 страницACE Personal Trainer Manual Chapter 13Đạt NguyễnОценок пока нет
- Adrenaline Surges in Myalgic Encephalomyelitis (M.E.)Документ10 страницAdrenaline Surges in Myalgic Encephalomyelitis (M.E.)zzirf100% (1)
- 50 Recovery From CFSДокумент189 страниц50 Recovery From CFSMaxime DesrosiersОценок пока нет
- Occupational Therapy and Chronic Fatigue SyndromeДокумент196 страницOccupational Therapy and Chronic Fatigue SyndromeMignonette Lorainne Atienza AbaoОценок пока нет
- Burnout, Fatigue, ExhaustionДокумент311 страницBurnout, Fatigue, ExhaustionDiana Ehlers100% (1)
- Kirlian Photograpy and Energy TappingДокумент7 страницKirlian Photograpy and Energy Tappingnblack3335140Оценок пока нет
- Effect of High Dose Vitamin C On Epstein-Barr Viral InfectionДокумент8 страницEffect of High Dose Vitamin C On Epstein-Barr Viral InfectionFilipos ConstantinОценок пока нет
- Comparison - VA Gulf War Research Strategic Plan As Revised by VA Staff - 05-31-2012Документ69 страницComparison - VA Gulf War Research Strategic Plan As Revised by VA Staff - 05-31-2012Anthony HardieОценок пока нет
- 2022-Sep-10 New Scientist - Figuring Out FatigueДокумент5 страниц2022-Sep-10 New Scientist - Figuring Out FatigueRyan HoangОценок пока нет
- Yogic Cure For ArthritiesДокумент59 страницYogic Cure For Arthritiesstar893190Оценок пока нет
- Paperpile - May 07 JSON ExportДокумент31 страницаPaperpile - May 07 JSON ExportMeaghan LinhartОценок пока нет
- CFS Research Long CovidДокумент122 страницыCFS Research Long CovidNikhil BhaskaranОценок пока нет
- Ebook PDF Contested Illness in Context An Interdisciplinary Study in Disease Definition PDFДокумент47 страницEbook PDF Contested Illness in Context An Interdisciplinary Study in Disease Definition PDFflorence.padilla424100% (39)
- SAT Writing - ParallelismДокумент25 страницSAT Writing - ParallelismBipan NeupaneОценок пока нет
- Cognitive and PsychologicalДокумент23 страницыCognitive and PsychologicalIsabel ValdésОценок пока нет
- UNIT 3 Symptoms!Документ29 страницUNIT 3 Symptoms!TaraaОценок пока нет
- PREFACE: " Chronic Fatigue Syndrome: A Guide To The Homeopathic Treatment of CFS/M.E."Документ5 страницPREFACE: " Chronic Fatigue Syndrome: A Guide To The Homeopathic Treatment of CFS/M.E."Diane SolomonОценок пока нет
- BSI BibДокумент41 страницаBSI BibdrmssОценок пока нет
- Mja 250553Документ6 страницMja 250553Marcelita DuwiriОценок пока нет
- Arousal Scoring - ASSMДокумент21 страницаArousal Scoring - ASSMkawaiiriceОценок пока нет