Вам также может понравиться
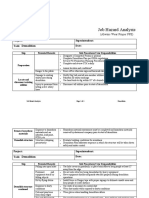
- Job Hazard Analysis DemolishДокумент4 страницыJob Hazard Analysis Demolishyajid bustomiОценок пока нет
- Fall Protection Equipment Inspection ChecklistДокумент2 страницыFall Protection Equipment Inspection ChecklistCristinaОценок пока нет
- Presentation On Work-Life BalanceДокумент41 страницаPresentation On Work-Life Balancekeyur5864% (14)
- Lone Working PolicyДокумент22 страницыLone Working PolicyVictor TasieОценок пока нет
- Risk Assessment ActivityДокумент5 страницRisk Assessment ActivityHarthwell CapistranoОценок пока нет
- 2.8 HSE Training MatrixДокумент2 страницы2.8 HSE Training MatrixMuhammad HassaanОценок пока нет
- Night Work Inspection ChecklistДокумент1 страницаNight Work Inspection ChecklistAdarsh sОценок пока нет
- HLTWHS005 - Conduct Manual Tasks SafelyДокумент4 страницыHLTWHS005 - Conduct Manual Tasks SafelyCourtney Holgate100% (1)
- Inspection - Forms - Lanyard - Body HardnessДокумент1 страницаInspection - Forms - Lanyard - Body Hardnesspetrus jacobОценок пока нет
- Project:: SWP For Safe Use of MewpsДокумент3 страницыProject:: SWP For Safe Use of MewpsVaradaraju ThirunavukkarasanОценок пока нет
- Coshh: Risk Assessment No Product NameДокумент2 страницыCoshh: Risk Assessment No Product NameshameerОценок пока нет
- Man Basket Cert 7101Документ1 страницаMan Basket Cert 7101Mac-Ross Cordova100% (1)
- BDCON833302 - Preliminary PagesДокумент5 страницBDCON833302 - Preliminary PagesStelito JumaranОценок пока нет
- FORM-03-OHSE-08 General Work Permit (GWP)Документ2 страницыFORM-03-OHSE-08 General Work Permit (GWP)Fadil MuhammadОценок пока нет
- Toolbox Talk - Traffic ManagementДокумент2 страницыToolbox Talk - Traffic ManagementAdrianОценок пока нет
- Standard Lift Plan TemplateДокумент2 страницыStandard Lift Plan TemplateInbarajОценок пока нет
- RESP. # 4 - Risk Assessment Guidelines IndexДокумент198 страницRESP. # 4 - Risk Assessment Guidelines IndexJay Omana0% (1)
- Risk Assessment Carpentry Works For Dismantling Wooden BoxesДокумент10 страницRisk Assessment Carpentry Works For Dismantling Wooden BoxesSinaОценок пока нет
- SPI HSE FR 02 Tower Erection ChecklistДокумент1 страницаSPI HSE FR 02 Tower Erection ChecklistChandan KumarОценок пока нет
- Safety Harness Monthly Checklist-Register JAN23Документ1 страницаSafety Harness Monthly Checklist-Register JAN23Iqbal HossainОценок пока нет
- 1 Hse Management ResponsibilityДокумент13 страниц1 Hse Management ResponsibilityRATAN BHATIAОценок пока нет
- Doshm Semester 6 Final Examination - Hirarc Presentation: Students' Name: ID No: Batch No: Company Name (OJT Workplace)Документ27 страницDoshm Semester 6 Final Examination - Hirarc Presentation: Students' Name: ID No: Batch No: Company Name (OJT Workplace)Afiq IrsyadОценок пока нет
- INSP1 MobileCraneDailyInspectionДокумент1 страницаINSP1 MobileCraneDailyInspectionFuzail Ayaz100% (1)
- 3 CPCCCA3008 Student Learning Guide - Activity WorkbookДокумент83 страницы3 CPCCCA3008 Student Learning Guide - Activity WorkbookDRSSONIA11MAY SHARMAОценок пока нет
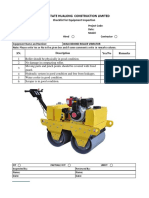
- Inspection Sheet For Roller and ConveyorДокумент2 страницыInspection Sheet For Roller and ConveyorPaintsil BrightОценок пока нет
- Module 7 - NC II - Practicing OSH Policies and Procedures - FinalДокумент80 страницModule 7 - NC II - Practicing OSH Policies and Procedures - FinalPS TCОценок пока нет
- Salary Slip SampleДокумент21 страницаSalary Slip Samplesantosh pathakОценок пока нет
- Inspection Checklist NGS12 - GCN02Документ5 страницInspection Checklist NGS12 - GCN02El D GraciaОценок пока нет
- Employee Timesheet Template: Or, Click Here To Create A Timesheet in SmartsheetДокумент11 страницEmployee Timesheet Template: Or, Click Here To Create A Timesheet in SmartsheetObedCorneliusJr.Оценок пока нет
- CPCCCM1015A Student Learning GuideДокумент43 страницыCPCCCM1015A Student Learning GuideAditya SharmaОценок пока нет
- PRO422 Safety SignageДокумент7 страницPRO422 Safety SignageAsyraf HakeemОценок пока нет
- CPCCSF2003A Cut and Bend Materials Using Oxy LPG Equipment LR V1Документ141 страницаCPCCSF2003A Cut and Bend Materials Using Oxy LPG Equipment LR V1FfdsfdsОценок пока нет
- Niversity of Eicester: P W P R E & F M DДокумент27 страницNiversity of Eicester: P W P R E & F M DFOZCANОценок пока нет
- RIICTT302D Conduct Impact Moling Ramming and Augering LR V1Документ135 страницRIICTT302D Conduct Impact Moling Ramming and Augering LR V1FfdsfdsОценок пока нет
- TSTI FormДокумент2 страницыTSTI FormJinu ThomasОценок пока нет
- Weekly HSE inspection checklist for Balewadi projectsДокумент2 страницыWeekly HSE inspection checklist for Balewadi projectsalvhyan anandolakiОценок пока нет
- CPCCWHS1001 - Prepare To Work Safely in The Construction IndustryДокумент4 страницыCPCCWHS1001 - Prepare To Work Safely in The Construction IndustryCourtney HolgateОценок пока нет
- Firefighting PDFДокумент78 страницFirefighting PDFf.B100% (1)
- L4W - TLILIC2001A - Information Booklet - V4 PDFДокумент54 страницыL4W - TLILIC2001A - Information Booklet - V4 PDFdulshanОценок пока нет
- Cpccohs2001a - Module 1Документ32 страницыCpccohs2001a - Module 1Nazareno BalagaОценок пока нет
- E-Fact 02 - Preventing Vehicle Accidents in ConstructionДокумент9 страницE-Fact 02 - Preventing Vehicle Accidents in ConstructionAntonio LeiteОценок пока нет
- Inspect SRL for SafetyДокумент1 страницаInspect SRL for Safetyghifariaghnia0% (1)
- PSB-221 Worker Hit by A Reversing VehicleДокумент1 страницаPSB-221 Worker Hit by A Reversing Vehiclejayand_netОценок пока нет
- 20159Документ220 страниц20159Kaso HasanОценок пока нет
- Painting, Taping, Texturing or Epoxy CoatingsДокумент1 страницаPainting, Taping, Texturing or Epoxy CoatingsHenryOdohОценок пока нет
- Heavy Equipment Safety WarningsДокумент2 страницыHeavy Equipment Safety Warningswillh00p3rОценок пока нет
- EQUIPMENT CHECKLISTДокумент4 страницыEQUIPMENT CHECKLISTBharathi SilambarasanОценок пока нет
- Ppe Issue RegisterДокумент1 страницаPpe Issue RegisterAnsarMahmoodОценок пока нет
- Movable Tower Light-Monthly Inspection Checklist: Acceptable Not Acceptable N/AДокумент1 страницаMovable Tower Light-Monthly Inspection Checklist: Acceptable Not Acceptable N/Amunna yadav100% (1)
- Manual Kestrel 5400Документ24 страницыManual Kestrel 5400Larissa JaramilloОценок пока нет
- 980 Behavior Based Safety Program PDFДокумент2 страницы980 Behavior Based Safety Program PDFherik0% (1)
- Site Safety Meeting AgendaДокумент2 страницыSite Safety Meeting AgendaMohamad Hidayat Zainul Masri100% (2)
- Lesson Learned-HIPO Near Miss - Energy IsolationДокумент1 страницаLesson Learned-HIPO Near Miss - Energy IsolationMukeshОценок пока нет
- MSAENV272 Sample Assessment ResourceДокумент16 страницMSAENV272 Sample Assessment ResourceShakthi ThiyageswaranОценок пока нет
- Form-062-Pre Start Daily Lifting ChecklistДокумент1 страницаForm-062-Pre Start Daily Lifting ChecklistJishad NalakathОценок пока нет
- Lifting Operations: Best Practice GuideДокумент16 страницLifting Operations: Best Practice GuideuknandiОценок пока нет
- Assessment Cover Sheet: (Print All Details and Attach To Front of Assessment Task/assignment Before Submitting)Документ18 страницAssessment Cover Sheet: (Print All Details and Attach To Front of Assessment Task/assignment Before Submitting)PieОценок пока нет
- Student Learning Guide PDF enДокумент34 страницыStudent Learning Guide PDF enTianna FrancisОценок пока нет
- Ocp BatchingДокумент1 страницаOcp BatchingAarya Mishra TiwariОценок пока нет
- Plywood Material Safety Data Sheet For MR Plywood PDFДокумент4 страницыPlywood Material Safety Data Sheet For MR Plywood PDFNirvana NircisОценок пока нет
- Dump TruckДокумент4 страницыDump TruckHugo RodriguezОценок пока нет
- Module 1 (LOTO Introduction)Документ33 страницыModule 1 (LOTO Introduction)ErnestoОценок пока нет
- Lifts and Lifting Equipment Policy and Best Practice NoteДокумент30 страницLifts and Lifting Equipment Policy and Best Practice NoteAnsara Pasir TumbohОценок пока нет
- OMC PTW LiftingДокумент2 страницыOMC PTW LiftingKarthik KarunanithiОценок пока нет
- EHS 2-F8 PTW LiftingДокумент2 страницыEHS 2-F8 PTW LiftingLee Xiao YuОценок пока нет
- Fire WatchДокумент7 страницFire WatchMateo RosasОценок пока нет
- SDS Titanium-Dioxide TIONA 59Документ7 страницSDS Titanium-Dioxide TIONA 59alfa twoОценок пока нет
- Business Essentials: Ebert, Griffin, Starke, DracopoulosДокумент41 страницаBusiness Essentials: Ebert, Griffin, Starke, DracopoulosAlexandru ConstantinОценок пока нет
- Global Working Conditions Guidance StatementsДокумент1 страницаGlobal Working Conditions Guidance StatementsMarwan HafizОценок пока нет
- TTT Presentation SlidesДокумент16 страницTTT Presentation SlidesSyed HusseinОценок пока нет
- Job Hazard Analysis Excavation and OthersДокумент8 страницJob Hazard Analysis Excavation and OthersJurgen MarangaОценок пока нет
- Safety Data Sheet: SECTION 1: Identification of The Substance/mixture and of The Company/undertakingДокумент9 страницSafety Data Sheet: SECTION 1: Identification of The Substance/mixture and of The Company/undertakingeadriesОценок пока нет
- Assessment of Health RisksДокумент27 страницAssessment of Health RisksMohamed GHAFFARОценок пока нет
- Safety Data Sheet: Sea SatinДокумент8 страницSafety Data Sheet: Sea SatinJessik CerónОценок пока нет
- NEBOSH International General Certificate in Occupational Safety and HealthДокумент5 страницNEBOSH International General Certificate in Occupational Safety and Healthوأكثرهم كارهونОценок пока нет
- Multi-Purpose Grease SDSДокумент15 страницMulti-Purpose Grease SDSSULAEMAN FAJRIОценок пока нет
- Know OHS Signs & RulesДокумент20 страницKnow OHS Signs & RulesDaniel BognotОценок пока нет
- Labour Law SyllabuДокумент4 страницыLabour Law Syllaburmbj94_scribdОценок пока нет
- SHE App 13 - HCS ControllerДокумент2 страницыSHE App 13 - HCS ControllerMunaku TafadzwaОценок пока нет
- Workshop On Advanced Ergonomics Risk AssessmentДокумент115 страницWorkshop On Advanced Ergonomics Risk AssessmentIma HishamОценок пока нет
- F03 Vendor Quarterly Compliance InspectionДокумент2 страницыF03 Vendor Quarterly Compliance Inspectionsalman ahmedОценок пока нет
- Hse Plan - SFMGCДокумент39 страницHse Plan - SFMGCthalaimalai817Оценок пока нет
- Compensation and BenefitsДокумент4 страницыCompensation and BenefitsNiño Sismoan BenigayОценок пока нет
- Rimula x30Документ7 страницRimula x30hastaОценок пока нет
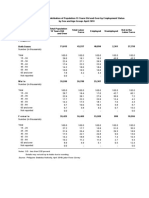
- TABLE 1 Percent Distribution of Population 15 Years Old and Over by Employment Status by Sex and Age Group April 2018Документ19 страницTABLE 1 Percent Distribution of Population 15 Years Old and Over by Employment Status by Sex and Age Group April 2018RoxanОценок пока нет
- Safety Data Sheet: Metalcrete IndustriesДокумент4 страницыSafety Data Sheet: Metalcrete IndustriesCarlos Alberto Luyo BuendíaОценок пока нет
- HIRARC ELECTRICAL WORK DoneДокумент1 страницаHIRARC ELECTRICAL WORK DoneAhmad Muhammad Yahya Bin Abdul TaibОценок пока нет
- Leave W/ Pay Leave W/ Pay Holiday Pay Holiday Pay: Total Deductions Total DeductionsДокумент1 страницаLeave W/ Pay Leave W/ Pay Holiday Pay Holiday Pay: Total Deductions Total DeductionsVic CumpasОценок пока нет