Вам также может понравиться
- DR Form - Cerbito PrintДокумент3 страницыDR Form - Cerbito PrintMelodyJane CerbitoОценок пока нет
- Actual Delivery In: St. Anthony'S CollegeДокумент2 страницыActual Delivery In: St. Anthony'S CollegeNicolne LorraineОценок пока нет
- Actual Delivery FormДокумент1 страницаActual Delivery FormGilyan ZaniahОценок пока нет
- PRC FORM To Be SubmittedДокумент6 страницPRC FORM To Be SubmittedCarlos NiñoОценок пока нет
- University of San CarlosДокумент8 страницUniversity of San CarlosEych DeeОценок пока нет
- Case Form IsuДокумент5 страницCase Form IsuJamesОценок пока нет
- ODC FORM 1 KoДокумент10 страницODC FORM 1 KoNiNyo HabunganОценок пока нет
- Print Perlas FormДокумент3 страницыPrint Perlas FormSuzette PerlasОценок пока нет
- Record of Actual Deliveries Handled Record of Actual Delivery HandledДокумент10 страницRecord of Actual Deliveries Handled Record of Actual Delivery HandledYvannah Joy BasanesОценок пока нет
- PRC FORMS 1 1 2 1Документ8 страницPRC FORMS 1 1 2 1AhrisJeannine EscuadroОценок пока нет
- PRC 2Документ5 страницPRC 2Yendor Medalle PickeringОценок пока нет
- Operating Room Form (Major and Minor) : University of The VisayasДокумент16 страницOperating Room Form (Major and Minor) : University of The VisayasJohn Mitchelle NОценок пока нет
- Odc Form 2aДокумент5 страницOdc Form 2aquiabenjchОценок пока нет
- Baho PutayДокумент3 страницыBaho PutayLorraine Nicolne B. CortejoОценок пока нет
- Southwestern University - PRC FormatДокумент15 страницSouthwestern University - PRC FormatemythereseОценок пока нет
- Procedure Performed: Hospital/Home/Lying-in Clinic, Municipality/City/ProvinceДокумент5 страницProcedure Performed: Hospital/Home/Lying-in Clinic, Municipality/City/ProvincejefzisgoodОценок пока нет
- Arpon MDL Actual SRCH PDFДокумент1 страницаArpon MDL Actual SRCH PDFMilcah BartolomeОценок пока нет
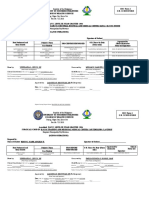
- Colegio San Agustin - Bacolod College of Health and Allied ProfessionsДокумент1 страницаColegio San Agustin - Bacolod College of Health and Allied ProfessionsJmarie Brillantes PopiocoОценок пока нет
- Final PRC DR Sample TemplateДокумент4 страницыFinal PRC DR Sample TemplatenovelloveОценок пока нет
- PRC Form New Format 2010 Western Mindanao State UniversityДокумент5 страницPRC Form New Format 2010 Western Mindanao State UniversityjefzisgoodОценок пока нет
- TemplatesДокумент10 страницTemplatesmagicnikkiОценок пока нет
- World Citi Colleges: Actual Delivery in - Batasan Lying-In, Quezon CityДокумент2 страницыWorld Citi Colleges: Actual Delivery in - Batasan Lying-In, Quezon CityG FernandezОценок пока нет
- Or DR Summary CasesДокумент5 страницOr DR Summary CasesAndrian BunaОценок пока нет
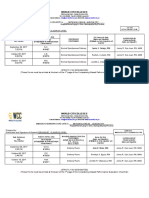
- Northern Christian College Nursing Students Clinical ExperiencesДокумент4 страницыNorthern Christian College Nursing Students Clinical ExperiencesSheryl Ann Barit PedinesОценок пока нет
- Scrub Forms NewДокумент6 страницScrub Forms Newbluenurse88Оценок пока нет
- CN Actual - GPH - CorcinoДокумент1 страницаCN Actual - GPH - CorcinoJohn Robert CorcinoОценок пока нет
- Arpon MDL Newborn PDFДокумент1 страницаArpon MDL Newborn PDFMilcah BartolomeОценок пока нет
- Scrub FormsДокумент6 страницScrub FormsnoeljrpajaresОценок пока нет
- Rustom Jhon MaestreДокумент4 страницыRustom Jhon MaestreAsdfghjlОценок пока нет
- TEMPLATES LastДокумент6 страницTEMPLATES LastZhy CaluzaОценок пока нет
- Republic of The Philippines: ODC Form 1 O.R. Scrub FormДокумент8 страницRepublic of The Philippines: ODC Form 1 O.R. Scrub FormghelzoneОценок пока нет
- Case Slip DRДокумент4 страницыCase Slip DRCalimlim KimОценок пока нет
- ODC Form 2B Surgical Sub Internship ReportДокумент1 страницаODC Form 2B Surgical Sub Internship ReportDwyane JamesОценок пока нет
- Hardam Furigay Colleges Foundation Inc. Board of Midwifery: Republic of The PhilippinesДокумент15 страницHardam Furigay Colleges Foundation Inc. Board of Midwifery: Republic of The Philippinesjohn_esturcoОценок пока нет
- Actual DeliveryДокумент1 страницаActual DeliveryNevea CariñoОценок пока нет
- DR Cases FormДокумент3 страницыDR Cases FormCyrus GarciaОценок пока нет
- Major Circu BlankДокумент2 страницыMajor Circu BlankAizha Noelle CataminОценок пока нет
- Actual DeliveryДокумент1 страницаActual Deliverygarceniego29Оценок пока нет
- PRC Form No.Документ10 страницPRC Form No.Yvannah Joy Basanes100% (1)
- ODC Form Delivery RecordsДокумент5 страницODC Form Delivery RecordsRobert Ross DulayОценок пока нет
- ODC FORM AnnaДокумент10 страницODC FORM AnnaDaywalker PedragozaОценок пока нет
- 4thyr. ZCMC Scrub MinorДокумент1 страница4thyr. ZCMC Scrub MinorLey BeltranОценок пока нет
- Circu-O RДокумент1 страницаCircu-O RSanny RamosОценок пока нет
- Ateneo Zamboanga Nursing FormsДокумент17 страницAteneo Zamboanga Nursing FormsRyan MirandaОценок пока нет
- Guiwan Main Health Center and Lying-In Clinic, Zamboanga CityДокумент17 страницGuiwan Main Health Center and Lying-In Clinic, Zamboanga CityRyan MirandaОценок пока нет
- Manila Tytana CollegesДокумент1 страницаManila Tytana CollegesSkyeОценок пока нет
- NBC TagudinДокумент1 страницаNBC TagudinMiling-miling ChorawanОценок пока нет
- Sheryl Ann B. Pedines: The Institution For Better LifeДокумент4 страницыSheryl Ann B. Pedines: The Institution For Better LifeSheryl Ann Barit PedinesОценок пока нет
- Print Ko BukasДокумент3 страницыPrint Ko BukasKatrina CaveОценок пока нет
- Hamida Haron CaseДокумент5 страницHamida Haron CasegadzОценок пока нет
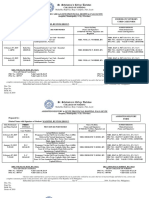
- St. Anthony College delivery recordsДокумент3 страницыSt. Anthony College delivery recordsMaristelaMolinaОценок пока нет
- Midwives CasesДокумент4 страницыMidwives CasesRhea LynОценок пока нет
- Intern'S Personal Data Sheet Personal DataДокумент10 страницIntern'S Personal Data Sheet Personal DataPenn YcongОценок пока нет
- Nursing college delivers quality careДокумент4 страницыNursing college delivers quality careJustine Rs Dela TorreОценок пока нет
- Turco Ched Forms 4Документ9 страницTurco Ched Forms 4Eyanah Delos ReyesОценок пока нет
- Regional Office: Dav Institutions, Odisha Zone-Ii Dr. A. N. Khosla Dav Public School, RourkelaДокумент2 страницыRegional Office: Dav Institutions, Odisha Zone-Ii Dr. A. N. Khosla Dav Public School, RourkelaRajat Kumar PadhanОценок пока нет
- Actual DRДокумент1 страницаActual DRSanny RamosОценок пока нет
- Certified Pediatric Emergency Nurse Review: Putting It All TogetherОт EverandCertified Pediatric Emergency Nurse Review: Putting It All TogetherОценок пока нет
- ExpatMD: Your Guide to Living and Working as a Physician in Australia and New ZealanОт EverandExpatMD: Your Guide to Living and Working as a Physician in Australia and New ZealanОценок пока нет
- Goal Achieved Grade Six Dropout to University Graduate In Papua New GuineaОт EverandGoal Achieved Grade Six Dropout to University Graduate In Papua New GuineaОценок пока нет
- Nurse Licensure Examination Review Center for Allied Professions (RCAPДокумент15 страницNurse Licensure Examination Review Center for Allied Professions (RCAPnikko0427Оценок пока нет
- Atls 1Документ5 страницAtls 1Mega MalyndaОценок пока нет
- Nursing Acn-IiДокумент80 страницNursing Acn-IiMunawar100% (6)
- Peace Corps Medical Officer (PCMO) Job AnnouncementДокумент3 страницыPeace Corps Medical Officer (PCMO) Job AnnouncementAccessible Journal Media: Peace Corps DocumentsОценок пока нет
- "We Are Their Slaves" by Gregory FlanneryДокумент4 страницы"We Are Their Slaves" by Gregory FlanneryAndy100% (2)
- Manajemen Pemeliharaan Puyuh Periode Layer Di CV Agri Bird Karanganyar Jawa TengahДокумент54 страницыManajemen Pemeliharaan Puyuh Periode Layer Di CV Agri Bird Karanganyar Jawa TengahRyah NurОценок пока нет
- UntitledДокумент221 страницаUntitledlaljadeff12Оценок пока нет
- Jakarta Cardiovascular Care Unit Network System OverviewДокумент52 страницыJakarta Cardiovascular Care Unit Network System OverviewekaОценок пока нет
- HIV Prevention: HSCI 225 BY Mutua Moses MuluДокумент23 страницыHIV Prevention: HSCI 225 BY Mutua Moses MuluJibril MohamudОценок пока нет
- Hand Injuries & Their ManagementsДокумент78 страницHand Injuries & Their ManagementsKuruОценок пока нет
- AFP Hemoptysis - 2022Документ9 страницAFP Hemoptysis - 2022Joshua DiaoОценок пока нет
- Iimplant AbutmentsДокумент8 страницIimplant AbutmentsDr. AtheerОценок пока нет
- Tinea IncognitoДокумент1 страницаTinea IncognitoJana AtanasovaОценок пока нет
- Nursing Audit ScheduleДокумент2 страницыNursing Audit ScheduleArvinjohn Gacutan0% (1)
- Vector and Pest Control in DisastersДокумент10 страницVector and Pest Control in DisastersTaufik RizkiandiОценок пока нет
- Drug in PregnancyДокумент5 страницDrug in PregnancyjokosudibyoОценок пока нет
- OGL 481 Pro-Seminar I: PCA-Ethical Communities Worksheet Erica KovarikДокумент4 страницыOGL 481 Pro-Seminar I: PCA-Ethical Communities Worksheet Erica Kovarikapi-529016443Оценок пока нет
- Ekstrak Kulit Buah Naga Super Merah Sebagai Anti-Kanker PayudaraДокумент5 страницEkstrak Kulit Buah Naga Super Merah Sebagai Anti-Kanker PayudaraWildatul Latifah IIОценок пока нет
- Addressing The Impact of Foster Care On Biological Children and Their FamiliesДокумент21 страницаAddressing The Impact of Foster Care On Biological Children and Their Familiesapi-274766448Оценок пока нет
- Cognidox - A Complete Guide To Medical Device DevelopmentДокумент38 страницCognidox - A Complete Guide To Medical Device DevelopmentcivicbladeОценок пока нет
- Immunization WHOДокумент17 страницImmunization WHOMuhammad Hardhantyo PuspowardoyoОценок пока нет
- 2.4 Maxillofacial Trauma (Sia) - Sales&TanДокумент11 страниц2.4 Maxillofacial Trauma (Sia) - Sales&Tanmr dojimamanОценок пока нет
- Anti-epileptic drugs: Types, Mechanisms & TreatmentДокумент7 страницAnti-epileptic drugs: Types, Mechanisms & TreatmentSampada ghodkiОценок пока нет
- HRFuture Sept 2020 MJLKJДокумент59 страницHRFuture Sept 2020 MJLKJGlecy KimОценок пока нет
- TOFPA: A Surgical Approach To Tetralogy of Fallot With Pulmonary AtresiaДокумент24 страницыTOFPA: A Surgical Approach To Tetralogy of Fallot With Pulmonary AtresiaRedmond P. Burke MD100% (1)
- CH 09Документ16 страницCH 09KittiesОценок пока нет
- Hazard Full SlideДокумент31 страницаHazard Full SlideRenKangWongОценок пока нет
- hf305 00 Dfu DeuДокумент54 страницыhf305 00 Dfu DeuMauro EzechieleОценок пока нет
- CBLM-BEAUTY CARE - FinalДокумент75 страницCBLM-BEAUTY CARE - FinalQuimby Quiano100% (3)
- Ontario Works Service Delivery Model CritiqueДокумент14 страницOntario Works Service Delivery Model CritiquewcfieldsОценок пока нет