Вам также может понравиться
- NCP Impaired SkinДокумент2 страницыNCP Impaired Skinarjay2306_obcq100% (1)
- Impaired Skin IntegrityДокумент2 страницыImpaired Skin IntegrityBesael BaccolОценок пока нет
- Impaired Physical Mobility...Документ3 страницыImpaired Physical Mobility...Christy BerryОценок пока нет
- NCP Impaired Skintissue IntegrityДокумент5 страницNCP Impaired Skintissue IntegrityArt Christian RamosОценок пока нет
- NCP For CHF 3 Activity IntoleranceДокумент2 страницыNCP For CHF 3 Activity IntoleranceAngelyn ArdinesОценок пока нет
- NCP For Impaired Physical MobilityДокумент1 страницаNCP For Impaired Physical Mobilityitzme_andreaОценок пока нет
- Deficit)Документ2 страницыDeficit)Lee DeeОценок пока нет
- NCP Near DrowningДокумент1 страницаNCP Near Drowningchristine louise bernardoОценок пока нет
- Compartment Syndrome NCP (PAIN)Документ2 страницыCompartment Syndrome NCP (PAIN)eunica16Оценок пока нет
- Self Care DeficitДокумент4 страницыSelf Care DeficitEllaine RamirezОценок пока нет
- NCP LymphedemaДокумент1 страницаNCP Lymphedemayasira50% (2)
- Word Ncp.......... TetanusДокумент6 страницWord Ncp.......... TetanusaianrОценок пока нет
- "Mayroong Namuong Dugo Sa Utak Niya Kaya Hindi Maayos Ang Daloy NG Dugo Rito" As Verbalized by The Patient'sДокумент4 страницы"Mayroong Namuong Dugo Sa Utak Niya Kaya Hindi Maayos Ang Daloy NG Dugo Rito" As Verbalized by The Patient'sAllisson BeckersОценок пока нет
- As Needed.: Environmental Stimuli 6Документ4 страницыAs Needed.: Environmental Stimuli 6Nicole GumolonОценок пока нет
- Activity Intolerance Related To AmeniaДокумент1 страницаActivity Intolerance Related To AmeniaSiti Syazana Mohamad MogriОценок пока нет
- NCP LocДокумент2 страницыNCP LocMel RodolfoОценок пока нет
- NCP OrthoДокумент6 страницNCP OrthoRuth Anne Arriesgado NañozОценок пока нет
- NCP For Mi PainДокумент2 страницыNCP For Mi PainKahMallariОценок пока нет
- NCP - Impaired Skin IntegrityДокумент1 страницаNCP - Impaired Skin Integrityjanelee28240% (2)
- NCP Delayed Wound RecoveryДокумент5 страницNCP Delayed Wound RecoveryDarkCeades100% (2)
- Post-Throidectomy Nursing Care PlanДокумент2 страницыPost-Throidectomy Nursing Care PlanCyrus De AsisОценок пока нет
- Ncp-Impaired S.i.-NavidasДокумент4 страницыNcp-Impaired S.i.-NavidasFran LanОценок пока нет
- NCP Impaired Skin IntegrityДокумент2 страницыNCP Impaired Skin IntegrityAshley Kate SantosОценок пока нет
- Impaired Physical Mobility RT Neuromuscular Skeletal Impairment.Документ3 страницыImpaired Physical Mobility RT Neuromuscular Skeletal Impairment.Abegail Abaygar100% (2)
- Risk For Impaired Skin IntegrityДокумент2 страницыRisk For Impaired Skin IntegrityKarl JoseОценок пока нет
- Nursing Diagnosis Risk For Impaired Skin IntegrityДокумент2 страницыNursing Diagnosis Risk For Impaired Skin IntegrityRazz Domenique Reyes Escaros100% (5)
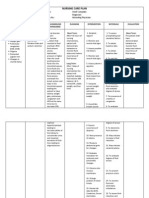
- NURSING CARE PLAN Problem Body Weakness Nursing Diagnosis Impaired PhysicalДокумент1 страницаNURSING CARE PLAN Problem Body Weakness Nursing Diagnosis Impaired Physicalmitchie riveraОценок пока нет
- Nursing Care PlanДокумент5 страницNursing Care Planruggero07100% (2)
- NCP For Impaired Skin IntegrityДокумент3 страницыNCP For Impaired Skin IntegrityAemz Alacasnap Ainegud100% (1)
- 6639burn NCPДокумент18 страниц6639burn NCPDivina Grace Renon Camba100% (1)
- Impaired Skin DMДокумент3 страницыImpaired Skin DMimnotdatsunny100% (1)
- NCP For CTTДокумент1 страницаNCP For CTTJen Rhae LimОценок пока нет
- Risk For InfectionДокумент3 страницыRisk For InfectioncamziiiОценок пока нет
- Activity IntoleranceДокумент3 страницыActivity Intolerancelouie roderos0% (1)
- Impaired Physical Mobility CholecystectomyДокумент2 страницыImpaired Physical Mobility CholecystectomyPrincess Danica Purcia100% (1)
- NCP BkaДокумент4 страницыNCP BkaKeeshia CesnerosОценок пока нет
- Worksheet#2-Maintaining Asepsis: Medical Asepsis Includes All Practices Intended To Confine A SpecificДокумент4 страницыWorksheet#2-Maintaining Asepsis: Medical Asepsis Includes All Practices Intended To Confine A SpecificCj MayoyoОценок пока нет
- Nursing Care Plan Acute Pain (Fronto-Temporal Mass)Документ2 страницыNursing Care Plan Acute Pain (Fronto-Temporal Mass)deric100% (1)
- NCP TetanusДокумент6 страницNCP Tetanusbjhilario100% (1)
- NCP (BODY WEAKNESS)Документ3 страницыNCP (BODY WEAKNESS)Jum ChumОценок пока нет
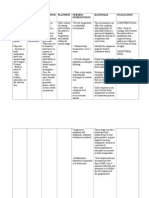
- Nursing Care Plan: Date/ Time Assessment Nursing Diagnosis Planning Intervention Evaluatio NДокумент2 страницыNursing Care Plan: Date/ Time Assessment Nursing Diagnosis Planning Intervention Evaluatio NnananaОценок пока нет
- Self Care DeficitДокумент3 страницыSelf Care DeficitAddie Labitad100% (2)
- NCP 1Документ1 страницаNCP 1hsiriaОценок пока нет
- NCP For SVTДокумент6 страницNCP For SVTRen VillenaОценок пока нет
- NCP Impaired Physical MobilityДокумент1 страницаNCP Impaired Physical MobilityCharmaine SolimanОценок пока нет
- Cancer Nursing Care Plan (NCP) - Risk For InfectionДокумент2 страницыCancer Nursing Care Plan (NCP) - Risk For InfectionAngie MandeoyaОценок пока нет
- Risk For Ineffective Tissue PerfusionДокумент5 страницRisk For Ineffective Tissue PerfusionElle Oranza100% (1)
- Skin IntegrityДокумент2 страницыSkin IntegrityJonica CamposОценок пока нет
- Impaired Verbal CommunicationДокумент6 страницImpaired Verbal CommunicationLaura Sansonetti100% (1)
- Risk For FallsДокумент1 страницаRisk For FallsEugene UCОценок пока нет
- NCP - Fluid RetentionДокумент3 страницыNCP - Fluid RetentionMichelle Teodoro100% (1)
- Student Nurses' Community: Nursing Care Plan AmputationДокумент3 страницыStudent Nurses' Community: Nursing Care Plan AmputationNur faizah bt azmiОценок пока нет
- Nursing Care Plan: CancerДокумент6 страницNursing Care Plan: Cancerneuronurse71% (7)
- Patriarca, Janna Mae H. Nursing Care Plan Client: Mr. YingДокумент1 страницаPatriarca, Janna Mae H. Nursing Care Plan Client: Mr. Yingjanna mae patriarca100% (2)
- NCP - Impaired Skin IntegrityДокумент3 страницыNCP - Impaired Skin IntegrityFlauros Ryu Jabien90% (30)
- College of Nursing and Allied Medical Sciences: WesleyanДокумент3 страницыCollege of Nursing and Allied Medical Sciences: WesleyanCharie OcampoОценок пока нет
- Nursing Care Plan: Clustered Cues Nursing Diagnosis Rationale Outcome Criteria Nursing Intervention Rationale EvaluationДокумент23 страницыNursing Care Plan: Clustered Cues Nursing Diagnosis Rationale Outcome Criteria Nursing Intervention Rationale EvaluationTweenie DalumpinesОценок пока нет
- Diabetes Mellitus: Assessment Diagnosis Planning Intervention Rationale EvaluationДокумент12 страницDiabetes Mellitus: Assessment Diagnosis Planning Intervention Rationale EvaluationDerick RanaОценок пока нет
- University of Luzon College of Nursing: Name - Jake Yvan DizonДокумент3 страницыUniversity of Luzon College of Nursing: Name - Jake Yvan DizonJake Yvan DizonОценок пока нет
- Impaired Skin IntegrityДокумент2 страницыImpaired Skin IntegrityBesael Baccol100% (1)
- Child AbuseДокумент51 страницаChild AbuseAmy Lalringhluani Chhakchhuak100% (5)
- Prelegere Osteoarticular enДокумент93 страницыPrelegere Osteoarticular enViorelVelenciucОценок пока нет
- ISRT Research Review 2008 KumpulanДокумент115 страницISRT Research Review 2008 KumpulanDwi Astika SariОценок пока нет
- Jsa For Pipe Laying Water and Sewer-1Документ8 страницJsa For Pipe Laying Water and Sewer-1Mikael Naqib83% (6)
- Jousting and The Medieval TournamentДокумент24 страницыJousting and The Medieval Tournamentthoth_sama100% (3)
- Lesions of Upper Motor Neurons and Lower Motor NeuronsДокумент9 страницLesions of Upper Motor Neurons and Lower Motor NeuronsJessy Ahmed El DamacyОценок пока нет
- Trigeminal NerveДокумент39 страницTrigeminal NerveKamlesh DuggaОценок пока нет
- Alcohol Intake: Increased Serum Amylase and Serum LipaseДокумент6 страницAlcohol Intake: Increased Serum Amylase and Serum LipaseJeffrey RamosОценок пока нет
- HemophiliaДокумент31 страницаHemophiliaspica25Оценок пока нет
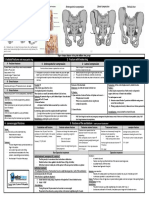
- Fracturte of Pelvis PDFДокумент2 страницыFracturte of Pelvis PDFYogi drОценок пока нет
- United States v. Carroll Towing Co.Документ2 страницыUnited States v. Carroll Towing Co.Madison MonzonОценок пока нет
- Long Form Yang StyleДокумент1 страницаLong Form Yang StylewestnorfolktaichiОценок пока нет
- MC0620179970 HDFC Life Group Credit Protect PlusДокумент8 страницMC0620179970 HDFC Life Group Credit Protect PlusAditya RajОценок пока нет
- Nervous SystemДокумент8 страницNervous SystemNicah FranciscoОценок пока нет
- Biomechanics Thefoot and Ankle UnitДокумент19 страницBiomechanics Thefoot and Ankle Unitshannithushan43Оценок пока нет
- Quotation: Furathama Ehee Training CentreДокумент5 страницQuotation: Furathama Ehee Training Centrehassan2020Оценок пока нет
- Gravaboi Codes and NumbersДокумент18 страницGravaboi Codes and NumbersHenrii Arias0% (1)
- Flail Chest MP Shah - CcuДокумент29 страницFlail Chest MP Shah - CcuMARTINОценок пока нет
- Canada Gateway MCC Qe Questions 1Документ100 страницCanada Gateway MCC Qe Questions 1Kak KfgaОценок пока нет
- Guide To Bodyweight TrainingДокумент271 страницаGuide To Bodyweight Trainingecstaticax100% (10)
- x=rcosθ y=rsinθ r = x + y θ = tan y xДокумент1 страницаx=rcosθ y=rsinθ r = x + y θ = tan y xmarkosОценок пока нет
- Lecture 9 - 2019Документ29 страницLecture 9 - 2019Eryn LIОценок пока нет
- Scxso 2222Документ1 страницаScxso 2222KateBarrionEspinosaОценок пока нет
- Sexual OffencesДокумент21 страницаSexual Offencesniraj_sdОценок пока нет
- Ma Gui Ba Gua Sample Exercise DocumentДокумент14 страницMa Gui Ba Gua Sample Exercise Documentshmoopiebear50% (2)
- Fall 1 Professional Development PlanДокумент9 страницFall 1 Professional Development Planapi-681176565Оценок пока нет
- Naziya & JignaДокумент44 страницыNaziya & Jignakishan100% (1)
- Edge of SurvivalДокумент502 страницыEdge of SurvivalRoman MoldoveanОценок пока нет
- Gen Intrs (Hockey)Документ24 страницыGen Intrs (Hockey)Rahul MahajanОценок пока нет
- 2-Sistem Otot 2Документ159 страниц2-Sistem Otot 2Vithya RamanathanОценок пока нет