Вам также может понравиться
- Family Health Assessment FormДокумент3 страницыFamily Health Assessment FormMitchTalledo100% (2)
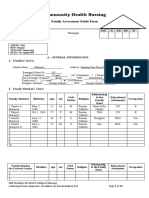
- Initial Data Base For Family Nursing PracticeДокумент9 страницInitial Data Base For Family Nursing PracticeAlyanna Crisologo100% (1)
- Family Structure, Characteristics and DynamicsДокумент6 страницFamily Structure, Characteristics and DynamicsErilyn Leigh ManaloОценок пока нет
- MMDST Multiple Choice Questionaires 2Документ13 страницMMDST Multiple Choice Questionaires 2Almera Rose Narce100% (1)
- Choral Speaking TextДокумент17 страницChoral Speaking Textlost78100% (2)
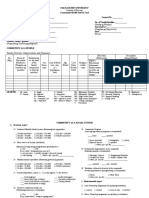
- Community Health Survey FormДокумент2 страницыCommunity Health Survey FormArvin Jon Bislig50% (2)
- DOH Programs Related To Family Health (EDITED)Документ93 страницыDOH Programs Related To Family Health (EDITED)Brix Valdriz100% (4)
- CHN Survey FormДокумент5 страницCHN Survey FormPʀɩŋcɘss LɩʌОценок пока нет
- #3 Family - Post Test 2Документ2 страницы#3 Family - Post Test 2Sheena Valenzuela75% (4)
- A Case Study Illustrating Nursing AssessmentДокумент9 страницA Case Study Illustrating Nursing AssessmentRozen ElizaldeОценок пока нет
- Standards of Public Health Nursing in The PhilippinesДокумент18 страницStandards of Public Health Nursing in The PhilippinesWilma BeraldeОценок пока нет
- Family Health NursingДокумент11 страницFamily Health NursingKBD100% (1)
- 2.2 - Recording and Reporting Based On FHSIS-noemi August25Документ40 страниц2.2 - Recording and Reporting Based On FHSIS-noemi August25Izæya80% (5)
- CHN Community Survey FormДокумент2 страницыCHN Community Survey FormRamyaj Odagor100% (1)
- Beginning Nurse's Role On Client Care PDFДокумент11 страницBeginning Nurse's Role On Client Care PDFulc100% (1)
- Selario Family Health Assessment FormДокумент7 страницSelario Family Health Assessment FormMaria Rosario Pangilinan SagmitОценок пока нет
- Family Nursing Typology (COPAR)Документ33 страницыFamily Nursing Typology (COPAR)Rhon Narciso100% (1)
- Family Nursing Care Plan: Initial Data BaseДокумент35 страницFamily Nursing Care Plan: Initial Data BaseEdraline LumawigОценок пока нет
- Typology of Nursing Problems in Family Nursing PracticeДокумент10 страницTypology of Nursing Problems in Family Nursing PracticeJustJ ThingsОценок пока нет
- PRC Bon Memorandum No.3s.08-Nle Amended GuidelinesДокумент8 страницPRC Bon Memorandum No.3s.08-Nle Amended GuidelinesSharyl Plan Saromines100% (1)
- Family Case AnalysisДокумент17 страницFamily Case Analysisapi-3832358100% (9)
- A Typology of Nursing Problems in Family Nursing PracticeДокумент10 страницA Typology of Nursing Problems in Family Nursing PracticeAnika Ajihil100% (2)
- Ortega - BSN2A - NCM 109 - Learning ActivityДокумент3 страницыOrtega - BSN2A - NCM 109 - Learning ActivityTrisha Faye OrtegaОценок пока нет
- Session Module DesignДокумент7 страницSession Module DesignLohrhen Lheighh CahreeniyowОценок пока нет
- Family Nursing ProcessДокумент7 страницFamily Nursing Processaibuty75% (4)
- Stress Provoking FactorsДокумент1 страницаStress Provoking Factorssleep whatОценок пока нет
- Family Nursing Care PlanДокумент34 страницыFamily Nursing Care PlanJai - Ho57% (14)
- Chapter 2 Chn2Документ26 страницChapter 2 Chn2Jahara Aiko PandapatanОценок пока нет
- FNCP 3rd Year 1st SemДокумент18 страницFNCP 3rd Year 1st SemJustin Reyes100% (1)
- FNCPДокумент10 страницFNCPMark Jaco AngОценок пока нет
- FNCP Maglaya FormatДокумент1 страницаFNCP Maglaya Formatjovanie01100% (6)
- Family Nursing ProcessДокумент25 страницFamily Nursing ProcessJAMES ROD MARINDUQUE100% (1)
- Home Visit OrientationДокумент29 страницHome Visit OrientationMay Chelle ErazoОценок пока нет
- Module 7 - DOH ProgramДокумент32 страницыModule 7 - DOH Programmirai desuОценок пока нет
- NCM 111 ModuleДокумент51 страницаNCM 111 ModuleCherry Ann DuranteОценок пока нет
- Family Health Nursing Practice 1Документ42 страницыFamily Health Nursing Practice 1Pam LalaОценок пока нет
- FNCP Poor Dental Health 2 (DONE)Документ3 страницыFNCP Poor Dental Health 2 (DONE)Mizchelle Angeles VilladorОценок пока нет
- First Level of AssessmentДокумент7 страницFirst Level of AssessmentJai - Ho100% (1)
- Family Health Nursing ProcessДокумент37 страницFamily Health Nursing ProcessNeethu Vincent100% (3)
- 2an - Chn-Family Interview Sheet - RamosДокумент8 страниц2an - Chn-Family Interview Sheet - RamosLouwella RamosОценок пока нет
- Family Nurse ContactДокумент10 страницFamily Nurse Contactphoebe100% (3)
- Community FNCP Complete 1Документ27 страницCommunity FNCP Complete 1Catherine Sinen ObinqueОценок пока нет
- Family Service and Progress Record (FSPR)Документ28 страницFamily Service and Progress Record (FSPR)Sarah Jane Magante100% (1)
- Family Nursing Care Plan Community DXДокумент59 страницFamily Nursing Care Plan Community DXSabrina Porquiado Magañan SNОценок пока нет
- Typology of Nursing Care ProblemsДокумент2 страницыTypology of Nursing Care ProblemsJohnny Yao JrОценок пока нет
- CHN Teaching PlanДокумент18 страницCHN Teaching Planfaith neoОценок пока нет
- Epi Brochure (Calalang)Документ2 страницыEpi Brochure (Calalang)Nickaela CalalangОценок пока нет
- Week 2 Rle ActivityДокумент3 страницыWeek 2 Rle ActivityMICHELLE BIANCA PATRICE CRUZОценок пока нет
- NCM 109 - Finals CompilationДокумент54 страницыNCM 109 - Finals CompilationMaria Kawilan100% (1)
- Ca 1 (Copar)Документ8 страницCa 1 (Copar)Roeder Max Pangramuyen0% (1)
- FNCP FinalДокумент28 страницFNCP FinalKristal Jane RuedasОценок пока нет
- Family Case Study-Chapter 6Документ6 страницFamily Case Study-Chapter 6Katherine 'Chingboo' Leonico LaudОценок пока нет
- Family Health Assessment FormДокумент6 страницFamily Health Assessment FormKlaire Dyn100% (1)
- Family Assessment ChecklistДокумент5 страницFamily Assessment ChecklistPauPauОценок пока нет
- INSTRUCTION: Please Provide The Answers To The Questions Below. No Questions Must Be Left Unanswered. ForДокумент6 страницINSTRUCTION: Please Provide The Answers To The Questions Below. No Questions Must Be Left Unanswered. ForNathaniel PulidoОценок пока нет
- CHN - Family Case StudyДокумент31 страницаCHN - Family Case Studyjohncarlo ramosОценок пока нет
- Survey Form (Baja, Joan R. BSN Ii-G)Документ32 страницыSurvey Form (Baja, Joan R. BSN Ii-G)Beverly DatuОценок пока нет
- Is/are Not Applicable, Kindly Write N/A.: UC-CON CHN Household Survey Form 1 - 7Документ7 страницIs/are Not Applicable, Kindly Write N/A.: UC-CON CHN Household Survey Form 1 - 7Loungayvan BatuyogОценок пока нет
- GROUP 2 Family Health Assessment FormДокумент6 страницGROUP 2 Family Health Assessment FormCassandra Grace Muerong Dela CruzОценок пока нет
- Household Survey Form 2Документ6 страницHousehold Survey Form 2HELLE AUBSОценок пока нет
- C.1 Estimated Average Family Income Per Month (Total Family Income: From A and B, Please Check) - C.2 Primary Source of LivelihoodДокумент6 страницC.1 Estimated Average Family Income Per Month (Total Family Income: From A and B, Please Check) - C.2 Primary Source of LivelihoodFavor ColaОценок пока нет
- Meat Processing Guide For Small BusinessДокумент7 страницMeat Processing Guide For Small BusinessBetz ChuiОценок пока нет
- Examen Parcial Inglés II - Percy Garcia Esquivel-2016Документ5 страницExamen Parcial Inglés II - Percy Garcia Esquivel-2016Yannina Lahisa PedrazaОценок пока нет
- Obsevations (All) FinalДокумент14 страницObsevations (All) FinalPhilip Griff EvansОценок пока нет
- GO Tamil Nadu Minimum Wage W.E.F April 1, 2018 To March 31, 2019Документ3 страницыGO Tamil Nadu Minimum Wage W.E.F April 1, 2018 To March 31, 2019Emerlson Moses0% (2)
- Camping - Make Your Own MRE's PDFДокумент9 страницCamping - Make Your Own MRE's PDFDarren Arnold100% (1)
- Margarita Cocktail Quest ResearchДокумент19 страницMargarita Cocktail Quest ResearchGeorge SinclairОценок пока нет
- 2018 Nutrition Intervention SnapshotДокумент1 страница2018 Nutrition Intervention SnapshotIrhamna Fauziah100% (1)
- Components of FoodДокумент8 страницComponents of FoodShaurya ManiktalaОценок пока нет
- Explosion Deep MineДокумент371 страницаExplosion Deep MineVincent J. CataldiОценок пока нет
- CLASS VIII Test Provim AnglishtДокумент2 страницыCLASS VIII Test Provim AnglishtSkerdi1Оценок пока нет
- Herbal TechnolgyДокумент33 страницыHerbal Technolgyashahmedn100% (1)
- 7 Science Exemplar Chapter 5Документ6 страниц7 Science Exemplar Chapter 5Tridasha AithalОценок пока нет
- The Importance of VitaminsДокумент3 страницыThe Importance of Vitaminskath_y88Оценок пока нет
- KSK PaddathiДокумент3 страницыKSK PaddathivtpsОценок пока нет
- FertilizerДокумент2 страницыFertilizerRyan DeMayОценок пока нет
- B.Inggris IPA-IPS P12 A PDFДокумент8 страницB.Inggris IPA-IPS P12 A PDFShella KhoiriyahОценок пока нет
- Rooti Farmaajo (Honeycomb Cheese Bread) Recipe - NYT CookingДокумент1 страницаRooti Farmaajo (Honeycomb Cheese Bread) Recipe - NYT CookingSara LamОценок пока нет
- Animals ReadingДокумент1 страницаAnimals ReadingMiguel Angel Acevedo MuentesОценок пока нет
- Past Simple and ContinuousДокумент7 страницPast Simple and Continuously miОценок пока нет
- Semisolid Dosage Forms: Industrial ProcessingДокумент35 страницSemisolid Dosage Forms: Industrial ProcessingSharon Fredric SinghОценок пока нет
- Food ItemsДокумент28 страницFood ItemsDr R P SinghОценок пока нет
- Mid Year Test 1 4 B WordДокумент4 страницыMid Year Test 1 4 B WordCarli PalumboОценок пока нет
- Radish Spinach BenefitsДокумент13 страницRadish Spinach BenefitsPoornima DineshОценок пока нет
- Introduction To SNAP: Policy BasicsДокумент8 страницIntroduction To SNAP: Policy BasicsPatricia DillonОценок пока нет
- Research Paper 5Документ15 страницResearch Paper 5api-270966663Оценок пока нет
- Techniques For Estimating Nutritive Values of FeedstuffsДокумент8 страницTechniques For Estimating Nutritive Values of FeedstuffsMuhammadHaseebОценок пока нет
- Onion Paste LWT PaperДокумент4 страницыOnion Paste LWT PaperYasir ArfatОценок пока нет
- Brain ChildДокумент2 страницыBrain ChildSohrab GhafoorОценок пока нет
- Food Services P&P PDFДокумент138 страницFood Services P&P PDFrajaakhaterОценок пока нет