Вам также может понравиться
- Form 3343Документ2 страницыForm 3343Harish ChandОценок пока нет
- BIOL10002 Lecture1 1 SlideДокумент45 страницBIOL10002 Lecture1 1 SlideLily RobinsonОценок пока нет
- Blanko Laboratorium BaruДокумент11 страницBlanko Laboratorium BaruYhan MarzukyОценок пока нет
- Simple Syrup Pesticide Report Findings 2016-2017Документ10 страницSimple Syrup Pesticide Report Findings 2016-2017Nitesh KumarОценок пока нет
- Sinta 4: Accredited: No. 230/E/KPT/2022Документ10 страницSinta 4: Accredited: No. 230/E/KPT/2022Mia KurniawatiОценок пока нет
- Lab Results Summary Under 40 CharactersДокумент1 страницаLab Results Summary Under 40 Characterslab rsmaleosorongОценок пока нет
- C T - US U SI U: Onversion Able Nits To NitsДокумент3 страницыC T - US U SI U: Onversion Able Nits To NitsEyob ayenachewОценок пока нет
- Diário de Saúde - AméliaДокумент1 страницаDiário de Saúde - AméliaheraclitocardosoОценок пока нет
- AS FoamДокумент5 страницAS Foammaria katherine pantojaОценок пока нет
- Chemcal - Mean of All InstrumentsДокумент1 страницаChemcal - Mean of All InstrumentsShoukrey AusmanОценок пока нет
- Cram Notes - Black BGДокумент20 страницCram Notes - Black BGbinjuОценок пока нет
- Meril 200 I: Test Name PositionДокумент2 страницыMeril 200 I: Test Name PositionAjeet YadavОценок пока нет
- Buffered Peptone Water - MerckДокумент5 страницBuffered Peptone Water - MerckMitha Arianti100% (1)
- LftДокумент1 страницаLftsirohisagar0001Оценок пока нет
- LFT RFT LP RBS EsrДокумент1 страницаLFT RFT LP RBS EsrDeepak SharmaОценок пока нет
- Pawan Gupta and Jitendra S. Sangwai: AbstractДокумент15 страницPawan Gupta and Jitendra S. Sangwai: AbstractLOLA PATRICIA MORALES DE LA CUBAОценок пока нет
- Avian Medicine:: Principles and ApplicationДокумент24 страницыAvian Medicine:: Principles and ApplicationAdriana PalmaОценок пока нет
- GDCAL - VS8577 - AMS - AFA06CA - Eng-Ita SAT 450 - 2021-04-22Документ1 страницаGDCAL - VS8577 - AMS - AFA06CA - Eng-Ita SAT 450 - 2021-04-22Trần Thanh ViệnОценок пока нет
- c230 PDFДокумент6 страницc230 PDFDewi susantiОценок пока нет
- Biokimia Sistem PencernaanДокумент29 страницBiokimia Sistem Pencernaan-Ryan Puriezo Chaniago-Оценок пока нет
- Non Energy Role of CarbohydratesДокумент34 страницыNon Energy Role of CarbohydratesDr. M. Prasad NaiduОценок пока нет
- Met Karbohidrat 3Документ57 страницMet Karbohidrat 3Khansa AliviaОценок пока нет
- Waste Water Test Report: SR No Parameters Unit ResultsДокумент1 страницаWaste Water Test Report: SR No Parameters Unit ResultsBhavik ZalaОценок пока нет
- Task ListДокумент3 страницыTask ListDinesh DhanavadeОценок пока нет
- Data Sheet: Certificate of Analysis Pooled Normal Human Male AB SerumДокумент2 страницыData Sheet: Certificate of Analysis Pooled Normal Human Male AB SerumKreative TechnolabsОценок пока нет
- Complete Water Quality AnalysisДокумент33 страницыComplete Water Quality AnalysisYahya IsiedОценок пока нет
- Buletin Lp.3Документ2 страницыBuletin Lp.3Joana B. NikolovaОценок пока нет
- SGLT2 InhibitorsДокумент47 страницSGLT2 InhibitorsGovind RankawatОценок пока нет
- Nilai Normal Pemeriksaan Kimia Klinik 2022Документ2 страницыNilai Normal Pemeriksaan Kimia Klinik 2022Icha NathaniaОценок пока нет
- Valores Calibrador PDFДокумент66 страницValores Calibrador PDFJoseCardonaОценок пока нет
- Form FU ICUДокумент2 страницыForm FU ICUErvaldi IlhamОценок пока нет
- Raju G (42Y/M) Liver Function Tests: Report For Tests AskedДокумент2 страницыRaju G (42Y/M) Liver Function Tests: Report For Tests AskedArun NaiduОценок пока нет
- Anugerah: Tanggal: No. Register Lab: Nama: Umur: Alamat: PengirimДокумент1 страницаAnugerah: Tanggal: No. Register Lab: Nama: Umur: Alamat: PengirimHakim Tanjung PrayogaОценок пока нет
- Liver Function Test (Lft-A)Документ4 страницыLiver Function Test (Lft-A)ce mgnregsОценок пока нет
- Citric Acid Cycle: The Central Energy PathwayДокумент57 страницCitric Acid Cycle: The Central Energy PathwayPridho GaziansyahОценок пока нет
- Daftar Nilai Kritis Laboratorium Yang Wajib Dilaporkan SegeraДокумент1 страницаDaftar Nilai Kritis Laboratorium Yang Wajib Dilaporkan SegeraNinik Indah KurniaОценок пока нет
- 1-Chronic Obstructive Pulmonary Disease - A Case ReportДокумент14 страниц1-Chronic Obstructive Pulmonary Disease - A Case Reportyakupkadri1945Оценок пока нет
- Lal Pathlabs ReportДокумент2 страницыLal Pathlabs ReportindianroadromeoОценок пока нет
- Lal Passthlabs ReportДокумент2 страницыLal Passthlabs ReportpramodkumarduvasuОценок пока нет
- Chapter 14 - BiomoleculesДокумент8 страницChapter 14 - BiomoleculesAvijeet NaiyaОценок пока нет
- Nilai Normal Mely LabДокумент3 страницыNilai Normal Mely LabRSU SAWIT INDAHОценок пока нет
- Design of Reverse Osmosis Desalination Plant in Suez CityДокумент10 страницDesign of Reverse Osmosis Desalination Plant in Suez CityAmr OkashaОценок пока нет
- Irma Water-Quality-Tables 2018 PDFДокумент12 страницIrma Water-Quality-Tables 2018 PDFviethuong96Оценок пока нет
- Lab FormДокумент23 страницыLab FormWiyanty NugrahaОценок пока нет
- Cambodia WQSДокумент2 страницыCambodia WQSNurwafaa AinaaОценок пока нет
- حل كتاب القسم كامل bio 102Документ46 страницحل كتاب القسم كامل bio 102Naba KhanОценок пока нет
- Department of BiochemistryДокумент1 страницаDepartment of BiochemistryBorn TO BE DEADОценок пока нет
- Examenes de LaboratorioДокумент1 страницаExamenes de LaboratorioJose Garcia MoranОценок пока нет
- Chapter 5 Food and Human NotesДокумент7 страницChapter 5 Food and Human Notes4107 曾凱謙 Tsang Hoi Him HymnОценок пока нет
- P15 - Navigating Treatment Frontiers - Optimizing Schizophrenia Treatment Through A Heretical Clozapine Cessation - A Forensic Psychiatry Case StudyДокумент1 страницаP15 - Navigating Treatment Frontiers - Optimizing Schizophrenia Treatment Through A Heretical Clozapine Cessation - A Forensic Psychiatry Case Studyangos.forensicОценок пока нет
- TriglyceridesДокумент2 страницыTriglyceridesAmmar MostafaОценок пока нет
- 562ue 2014-06Документ55 страниц562ue 2014-06vijayramaswamyОценок пока нет
- Instalasi Laboratorium Rsu Gmim Bethesda Tomohon Nilai Quality Control Harian Bulan: Parameter Target Range SatuanДокумент4 страницыInstalasi Laboratorium Rsu Gmim Bethesda Tomohon Nilai Quality Control Harian Bulan: Parameter Target Range SatuanCharles Bravo MaitОценок пока нет
- BlangkoДокумент4 страницыBlangkoParamitaОценок пока нет
- BIOCHEM VR ScriptsДокумент5 страницBIOCHEM VR ScriptsEla NavalesОценок пока нет
- Bang Tri So 2023-10-31Документ1 страницаBang Tri So 2023-10-31Nghi NguyenОценок пока нет
- PdfText - 2023-12-12T152233.242Документ2 страницыPdfText - 2023-12-12T152233.242joshipriya208Оценок пока нет
- Format Kimia DarahДокумент6 страницFormat Kimia DarahRSPN UnsyiahОценок пока нет
- Pga DLSJ ReviewДокумент6 страницPga DLSJ ReviewjenniОценок пока нет
- Corporate AgentsДокумент1 023 страницыCorporate AgentsVivek Thota0% (1)
- Agency Presentation - ZTCДокумент24 страницыAgency Presentation - ZTCHarish ChandОценок пока нет
- Mrs. Nirali Mehta: Insurance Proposal ForДокумент5 страницMrs. Nirali Mehta: Insurance Proposal ForHarish ChandОценок пока нет
- Jeevan Anand: Harish ChandДокумент4 страницыJeevan Anand: Harish ChandHarish ChandОценок пока нет
- Rad 28 E72Документ1 страницаRad 28 E72Harish ChandОценок пока нет
- Mr. Harish Chand: Presentation Specially Prepared ForДокумент4 страницыMr. Harish Chand: Presentation Specially Prepared ForHarish ChandОценок пока нет
- Jeevan Anand: Harish ChandДокумент4 страницыJeevan Anand: Harish ChandHarish ChandОценок пока нет
- 16 Year at 41 AgeДокумент4 страницы16 Year at 41 AgeHarish ChandОценок пока нет
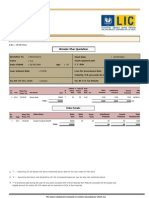
- Multi - Plan Chart: Harish ChandДокумент3 страницыMulti - Plan Chart: Harish ChandHarish ChandОценок пока нет
- Harish Chand: Jeevan Anand Plan PresentationДокумент4 страницыHarish Chand: Jeevan Anand Plan PresentationHarish ChandОценок пока нет
- Mr. Gupta: Insurance Proposal ForДокумент8 страницMr. Gupta: Insurance Proposal ForHarish ChandОценок пока нет
- Anmol Jeevan - 9811896425Документ1 страницаAnmol Jeevan - 9811896425Harish ChandОценок пока нет
- Rad 211 D0Документ1 страницаRad 211 D0Harish ChandОценок пока нет
- Mr. Gupta: Harish ChandДокумент4 страницыMr. Gupta: Harish ChandHarish ChandОценок пока нет
- Rad 20356Документ1 страницаRad 20356Harish ChandОценок пока нет
- All Illustration of LICДокумент6 страницAll Illustration of LICHarish ChandОценок пока нет
- Rad 1 FDF9Документ2 страницыRad 1 FDF9Harish ChandОценок пока нет
- Jeevan AkshayДокумент1 страницаJeevan AkshayHarish ChandОценок пока нет
- Rad 09206Документ3 страницыRad 09206Harish ChandОценок пока нет
- Rad 1 F405Документ3 страницыRad 1 F405Harish ChandОценок пока нет
- Rad 09206Документ3 страницыRad 09206Harish ChandОценок пока нет
- Jeevan Anand: Harish ChandДокумент4 страницыJeevan Anand: Harish ChandHarish ChandОценок пока нет
- Rad 1 F405Документ3 страницыRad 1 F405Harish ChandОценок пока нет
- Jeevan Anand: Harish ChandДокумент4 страницыJeevan Anand: Harish ChandHarish ChandОценок пока нет
- All Illustration of LICДокумент6 страницAll Illustration of LICHarish ChandОценок пока нет
- Jeevan Saral IllustrationДокумент3 страницыJeevan Saral IllustrationHarish ChandОценок пока нет
- Premiums Due Statement: Harish ChandДокумент1 страницаPremiums Due Statement: Harish ChandHarish ChandОценок пока нет
- Multi - Plan Chart: Harish ChandДокумент3 страницыMulti - Plan Chart: Harish ChandHarish ChandОценок пока нет
- Harish Chand: Multi - Plan ChartДокумент4 страницыHarish Chand: Multi - Plan ChartHarish ChandОценок пока нет
- Rad 09206Документ3 страницыRad 09206Harish ChandОценок пока нет
- Equipment Applications BTS 370Документ32 страницыEquipment Applications BTS 370oscacaiОценок пока нет
- Diasys Diagnostic Systems: Product CatalogДокумент55 страницDiasys Diagnostic Systems: Product CatalogpinciukassОценок пока нет
- Hyperlipidemia 1Документ32 страницыHyperlipidemia 1Binita ShakyaОценок пока нет
- LSAT and Mba Bank Exams PrelДокумент28 страницLSAT and Mba Bank Exams PrelSudip SinghОценок пока нет
- Turmeric: Nature'S Precious Medicine: Review ArticleДокумент7 страницTurmeric: Nature'S Precious Medicine: Review Articlechaitanya kumarОценок пока нет
- Lipoprotein MetabolismДокумент6 страницLipoprotein MetabolismVincent MwirigiОценок пока нет
- Clinical Pharmacy Answer Key-PINK PACOPДокумент29 страницClinical Pharmacy Answer Key-PINK PACOPKaguraОценок пока нет
- Preparation of Soyabean Milk and Its Comparison With Natural Milk 2Документ20 страницPreparation of Soyabean Milk and Its Comparison With Natural Milk 2RajatGupta100% (2)
- Diabetes Dan Penyakit Endokrin DR Sebastian JobulДокумент40 страницDiabetes Dan Penyakit Endokrin DR Sebastian JobulMiranda RozziqaОценок пока нет
- NRDP 201529Документ21 страницаNRDP 201529Zurielle LuboaОценок пока нет
- Saint Louis University Biochemistry Lab Exercises on Complex Lipids and Cholesterol MetabolismДокумент9 страницSaint Louis University Biochemistry Lab Exercises on Complex Lipids and Cholesterol MetabolismJudi Clarisse Bagano PaderesОценок пока нет
- Lipids: TEST(s) Normal UNIT(s)Документ1 страницаLipids: TEST(s) Normal UNIT(s)DrAssadullah HamzaОценок пока нет
- Pauling - The Vitamin C Theory of Heart Disease - by - Owen - FonorrowДокумент5 страницPauling - The Vitamin C Theory of Heart Disease - by - Owen - FonorrowAnonymous Jap77xvqPKОценок пока нет
- Nutrition Module 10Документ51 страницаNutrition Module 10SandeeОценок пока нет
- Sila Jawab SEMUA Soalan. Semua Jawapan Hendaklah Ditaip, Dilukis Secara Digital (Kecuali Gambar Yang Diminta) Dan Dihantar Dalam Format PDFДокумент7 страницSila Jawab SEMUA Soalan. Semua Jawapan Hendaklah Ditaip, Dilukis Secara Digital (Kecuali Gambar Yang Diminta) Dan Dihantar Dalam Format PDFJegathiswary GanasanОценок пока нет
- Blood Test PresentationДокумент129 страницBlood Test Presentationනුවන් චමීර ගුණවර්ධනОценок пока нет
- Amaranth Plant of The FutureДокумент118 страницAmaranth Plant of The FutureGabrIela PerezОценок пока нет
- LipoproteinsДокумент30 страницLipoproteinsApurba PradhanОценок пока нет
- Hair Cortisol and The Risk For Acute MyocardialДокумент10 страницHair Cortisol and The Risk For Acute MyocardialmizanОценок пока нет
- Jay Patrick Vitamin C ArticlesДокумент63 страницыJay Patrick Vitamin C ArticlesKrys Weaver0% (1)
- Volume: 04 Issue: 03 - May-Jun 2023: Central Asian Journal of Medical and Natural SciencesДокумент7 страницVolume: 04 Issue: 03 - May-Jun 2023: Central Asian Journal of Medical and Natural SciencesCentral Asian StudiesОценок пока нет
- Introduction To Clinical Health PsychologyДокумент271 страницаIntroduction To Clinical Health Psychologyshafijan100% (1)
- Fats Lecture NotesДокумент27 страницFats Lecture NotesyzaОценок пока нет
- (Lib24.vn) De-Thi-Thu-Thptqg-Nam-2017-Mon-Tieng-Anh-Th-S-Thanh-Hien-De-1Документ12 страниц(Lib24.vn) De-Thi-Thu-Thptqg-Nam-2017-Mon-Tieng-Anh-Th-S-Thanh-Hien-De-1Thu Ha NTОценок пока нет
- Price List ELITECH REAGEN 2015Документ3 страницыPrice List ELITECH REAGEN 2015sanggam tobingОценок пока нет
- Determination of Free Fatty Acids Report FinalisedДокумент7 страницDetermination of Free Fatty Acids Report FinalisedLAKHASTH JAYASILANОценок пока нет
- T1-2P1 MSДокумент28 страницT1-2P1 MSVladimir TrajanovikjОценок пока нет
- Fall 22 Week 5 General Meeting Ucla 101 LD WorkshopДокумент43 страницыFall 22 Week 5 General Meeting Ucla 101 LD Workshopapi-235454491Оценок пока нет
- Biochemical tests in diabetes: Glycated haemoglobin, glucose and creatinine analysisДокумент43 страницыBiochemical tests in diabetes: Glycated haemoglobin, glucose and creatinine analysisTRINEL ANGGRIATIОценок пока нет
- Dietray Fibers (Complete Lecture)Документ60 страницDietray Fibers (Complete Lecture)Nauman SattarОценок пока нет