Вам также может понравиться
- NCM 107 Activity 4-TabioloДокумент5 страницNCM 107 Activity 4-TabioloAce TabioloОценок пока нет
- Nursing Care PlanДокумент5 страницNursing Care PlanPaola Marie VenusОценок пока нет
- CP Intestinal Obstruction Nursing Care PlanДокумент7 страницCP Intestinal Obstruction Nursing Care PlanShiella Heart MalanaОценок пока нет
- MGH 8 - Ihd - NCPДокумент12 страницMGH 8 - Ihd - NCPSesinando Niez Quilao Jr.100% (1)
- Assessment Diagnosis Planning Nursing Intervention Rationale EvaluationДокумент2 страницыAssessment Diagnosis Planning Nursing Intervention Rationale Evaluationjennelyn losantaОценок пока нет
- Nursing Care PlanДокумент4 страницыNursing Care PlanJobelyn TunayОценок пока нет
- Health-Perception-Health-Management PatternДокумент3 страницыHealth-Perception-Health-Management PatternBela MillenaОценок пока нет
- NCPДокумент15 страницNCPCamille PinedaОценок пока нет
- Nursing Care PlanДокумент15 страницNursing Care PlanZhel Geron MercadoОценок пока нет
- NCP PTBДокумент6 страницNCP PTBJay Dela VegaОценок пока нет
- Hyperthermia and Risk For AspirationДокумент3 страницыHyperthermia and Risk For AspirationAlmyr RimandoОценок пока нет
- Nursing Care Plan Peptic UlcerДокумент3 страницыNursing Care Plan Peptic UlcerJefferson Baluyot PalmaОценок пока нет
- Rufino, Leslie Kriztel S. BSN 3-2 Group 1Документ6 страницRufino, Leslie Kriztel S. BSN 3-2 Group 1Deinielle Magdangal RomeroОценок пока нет
- Nursing Care Plan-1: Medical Diagnoses: Colorectal CancerДокумент2 страницыNursing Care Plan-1: Medical Diagnoses: Colorectal CancerBheru LalОценок пока нет
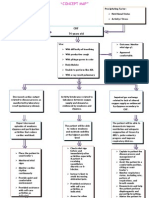
- Concept Map - Abby !Документ2 страницыConcept Map - Abby !Abegail Abaygar100% (3)
- Decreased Cardiac OutputДокумент4 страницыDecreased Cardiac OutputAdnan Khan100% (1)
- Word Ncp.......... TetanusДокумент6 страницWord Ncp.......... TetanusaianrОценок пока нет
- Case Report On Bipolar Affective Disorder: Mania With Psychotic SymptomsДокумент2 страницыCase Report On Bipolar Affective Disorder: Mania With Psychotic SymptomskslhfwoiebvОценок пока нет
- Assessment Nursing Diagnosis Planning Interventions EvaluationsДокумент4 страницыAssessment Nursing Diagnosis Planning Interventions EvaluationsAjay SupanОценок пока нет
- NCP PTBДокумент2 страницыNCP PTBMack Jhed AnarconОценок пока нет
- 7 Hyperthyroidism Nursing Care Plan (NCP)Документ1 страница7 Hyperthyroidism Nursing Care Plan (NCP)Apol PenОценок пока нет
- Nursing Care PlanДокумент6 страницNursing Care Plankreny1050% (2)
- Fistula NCPДокумент1 страницаFistula NCPHasna LisnaОценок пока нет
- Nursing Care Plan - Fatigue (Antepartum)Документ3 страницыNursing Care Plan - Fatigue (Antepartum)kaimimiyaОценок пока нет
- Assessment Diagnosis Planning Intrvention Rationale EvaluationДокумент1 страницаAssessment Diagnosis Planning Intrvention Rationale EvaluationMar OrdanzaОценок пока нет
- Drug-Study NCPДокумент5 страницDrug-Study NCPMURILLO, FRANK JOMARI C.Оценок пока нет
- Propranolol 1 PresentationДокумент17 страницPropranolol 1 Presentationapi-284092317100% (1)
- Acute PainДокумент3 страницыAcute PainJayr ChinОценок пока нет
- NCP BronchopneumoniaДокумент8 страницNCP BronchopneumoniaCrisantaCasliОценок пока нет
- Nursing Care Plan2Документ13 страницNursing Care Plan2Nna ANn CastleОценок пока нет
- HypertensionДокумент3 страницыHypertensionkarl de guzmanОценок пока нет
- Nursing Care Plan Cues Nursing Diagnosis Objective Intervention Rationale Evaluation SubjectiveДокумент2 страницыNursing Care Plan Cues Nursing Diagnosis Objective Intervention Rationale Evaluation SubjectiveFreisanChenMandumotanОценок пока нет
- PneumoniaДокумент2 страницыPneumoniaPia MedinaОценок пока нет
- Medication ThalassemiaДокумент3 страницыMedication ThalassemiaDivya ToppoОценок пока нет
- Nursing Care Plan: Assessment Diagnosis Planning Interventions Rationale EvaluationДокумент11 страницNursing Care Plan: Assessment Diagnosis Planning Interventions Rationale EvaluationDa NicaОценок пока нет
- NCP Acitivity IntoleranceДокумент3 страницыNCP Acitivity IntolerancegizelleОценок пока нет
- NCP 2 and Soapie 1Документ5 страницNCP 2 and Soapie 1narsD100% (1)
- Nursing Care Plan For Special ChildrenДокумент2 страницыNursing Care Plan For Special Childrenharas_dcsaisОценок пока нет
- Nanda NCP BasedДокумент14 страницNanda NCP Baseddeliejoyce100% (1)
- Acute Pain SCMCДокумент2 страницыAcute Pain SCMCWik Wik PantuaОценок пока нет
- Nursing Care PlanДокумент20 страницNursing Care PlanZamranosОценок пока нет
- NCPДокумент2 страницыNCPJamaica SaranquinОценок пока нет
- Nursing Care Plan: Risk For Disuse SyndromeДокумент2 страницыNursing Care Plan: Risk For Disuse SyndromeRozsy FakhrurОценок пока нет
- Subdural HematomaДокумент4 страницыSubdural Hematomarodamel gundanОценок пока нет
- Nursing Care Plan, Diagnosis, Interventions Hyperthermia, Fever, High TemperatureДокумент2 страницыNursing Care Plan, Diagnosis, Interventions Hyperthermia, Fever, High TemperatureVanessa AbboudОценок пока нет
- San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesДокумент3 страницыSan Francisco St. Butuan City 8600, Region XIII Caraga, Philippineskuro hanabusaОценок пока нет
- Nursing Care Plan Format Name: - Medical Diagnosis: - DateДокумент2 страницыNursing Care Plan Format Name: - Medical Diagnosis: - DateSheryl Ann Barit PedinesОценок пока нет
- As Needed.: Environmental Stimuli 6Документ4 страницыAs Needed.: Environmental Stimuli 6Nicole GumolonОценок пока нет
- NCP Set 1Документ18 страницNCP Set 1Augene Toribio50% (2)
- Assessment Diagnosis Planning Implementation Evaluation No Subjective Cues ObjectiveДокумент3 страницыAssessment Diagnosis Planning Implementation Evaluation No Subjective Cues ObjectiveMaverick LimОценок пока нет
- Head NurseДокумент11 страницHead Nursejannet20Оценок пока нет
- Knowledge DeficitДокумент5 страницKnowledge DeficitteamstrocaОценок пока нет
- AAAAA Altered-Body-Temp-NCPДокумент2 страницыAAAAA Altered-Body-Temp-NCPMoi ValdozОценок пока нет
- Case StudyДокумент12 страницCase StudyAllan Roy Malibiran BalderamaОценок пока нет
- Nursing Management of CVA and NIDDMДокумент12 страницNursing Management of CVA and NIDDMKaloy KamaoОценок пока нет
- Myocardial InfarctionДокумент5 страницMyocardial InfarctionDharline Abbygale Garvida AgullanaОценок пока нет
- IUFDДокумент13 страницIUFDChristopher Lontoc0% (1)
- NCP FinalДокумент18 страницNCP FinalJessica Medina100% (1)
- Conceptmaptext For EpДокумент9 страницConceptmaptext For Epapi-272402391Оценок пока нет
- NCP FinalДокумент7 страницNCP FinalAkira MizukamiОценок пока нет
- Age of Sigmar AoS - Battletome - Hedonites of Slaanesh - Errata 2023-01Документ4 страницыAge of Sigmar AoS - Battletome - Hedonites of Slaanesh - Errata 2023-01Ughu RajaОценок пока нет
- 2-Port Antenna Frequency Range Dual Polarization HPBW Adjust. Electr. DTДокумент5 страниц2-Port Antenna Frequency Range Dual Polarization HPBW Adjust. Electr. DTIbrahim JaberОценок пока нет
- Factor Affecting Child Dental Behaviour PedoДокумент19 страницFactor Affecting Child Dental Behaviour PedoFourthMolar.comОценок пока нет
- C Programming Bit Bank U-1, U-2Документ17 страницC Programming Bit Bank U-1, U-2HariahОценок пока нет
- Ezra Pound - PersonaeДокумент34 страницыEzra Pound - PersonaedanielrdzambranoОценок пока нет
- 555LДокумент8 страниц555LVictor Mamani VargasОценок пока нет
- Digital Image Processing Unit-8Документ4 страницыDigital Image Processing Unit-8Kpsteja TejaОценок пока нет
- The Manuals Com Cost Accounting by Matz and Usry 9th Edition Manual Ht4Документ2 страницыThe Manuals Com Cost Accounting by Matz and Usry 9th Edition Manual Ht4shoaib shakilОценок пока нет
- Derivative Pakistan PerspectiveДокумент99 страницDerivative Pakistan PerspectiveUrooj KhanОценок пока нет
- Individualism in Marketing CampaignДокумент6 страницIndividualism in Marketing CampaignTrần Nguyễn Khánh TrangОценок пока нет
- HOPE 2A MODULE 1 Introduction To SportsДокумент11 страницHOPE 2A MODULE 1 Introduction To SportsChristian Ray Lucnagan ReyesОценок пока нет
- Main CharacterДокумент5 страницMain CharacterFluffy RabbitОценок пока нет
- Roger Fidler DeclarationДокумент6 страницRoger Fidler Declarationnphillips0304Оценок пока нет
- WK5 SR MOD001074 Grundy 2006 PDFДокумент18 страницWK5 SR MOD001074 Grundy 2006 PDFadwiyahОценок пока нет
- Kebutuhan Modal Kerja Pada Cv. Cipta Karya Mandiri Di SamarindaДокумент7 страницKebutuhan Modal Kerja Pada Cv. Cipta Karya Mandiri Di SamarindaHerdi VhantОценок пока нет
- Case Study TemplateДокумент4 страницыCase Study Templateapi-355498849Оценок пока нет
- Amma Vun - Bala AshtagamДокумент4 страницыAmma Vun - Bala AshtagamSHIV RAMОценок пока нет
- Ed A 02.00 I 01Документ39 страницEd A 02.00 I 01Enrique BlancoОценок пока нет
- Begc133em20 21Документ14 страницBegc133em20 21nkОценок пока нет
- Title To GoodsДокумент2 страницыTitle To GoodsrrsinhanhpcОценок пока нет
- MSPM Clark UniversityДокумент27 страницMSPM Clark Universitytushar gargОценок пока нет
- Essay 1 John WatsonДокумент4 страницыEssay 1 John Watsonapi-259502356Оценок пока нет
- Carnatic Music NotationДокумент6 страницCarnatic Music Notationksenthil kumar100% (1)
- Student's Lab Pack: Preteens 02 11 Weeks CourseДокумент30 страницStudent's Lab Pack: Preteens 02 11 Weeks CourseMi KaОценок пока нет
- Automatic Water Level Indicator and Controller by Using ARDUINOДокумент10 страницAutomatic Water Level Indicator and Controller by Using ARDUINOSounds of PeaceОценок пока нет
- Fiche 2 ConnexionsДокумент2 страницыFiche 2 ConnexionsMaria Marinela Rusu50% (2)
- Definition of CultureДокумент14 страницDefinition of CultureRenee Louise CoОценок пока нет
- Joker Pattern PDF New PDFДокумент7 страницJoker Pattern PDF New PDFLorena CapogrossiОценок пока нет
- Aporte Al IPSS Del Empleador Por TrabajadorДокумент4 страницыAporte Al IPSS Del Empleador Por Trabajadorvagonet21Оценок пока нет
- Nonfiction Reading Test The Coliseum: Directions: Read The Following Passage and Answer The Questions That Follow. ReferДокумент3 страницыNonfiction Reading Test The Coliseum: Directions: Read The Following Passage and Answer The Questions That Follow. ReferYamile CruzОценок пока нет
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)От EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Рейтинг: 3 из 5 звезд3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionОт EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionРейтинг: 4 из 5 звезд4/5 (404)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОт EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОценок пока нет
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (32)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisОт EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisРейтинг: 4.5 из 5 звезд4.5/5 (42)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDОт EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDРейтинг: 5 из 5 звезд5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeРейтинг: 2 из 5 звезд2/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 4.5 из 5 звезд4.5/5 (82)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryОт EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryРейтинг: 4 из 5 звезд4/5 (46)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaОт EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsОт EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsРейтинг: 4 из 5 звезд4/5 (4)
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (6)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesОт EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesРейтинг: 4.5 из 5 звезд4.5/5 (1412)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsОт EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsРейтинг: 5 из 5 звезд5/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.От EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Рейтинг: 4.5 из 5 звезд4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityОт EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityРейтинг: 4 из 5 звезд4/5 (5)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsОт EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsРейтинг: 4.5 из 5 звезд4.5/5 (170)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisОт EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisРейтинг: 5 из 5 звезд5/5 (8)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisОт EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisРейтинг: 3.5 из 5 звезд3.5/5 (2)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessОт EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessРейтинг: 4.5 из 5 звезд4.5/5 (328)
- Troubled: A Memoir of Foster Care, Family, and Social ClassОт EverandTroubled: A Memoir of Foster Care, Family, and Social ClassРейтинг: 4.5 из 5 звезд4.5/5 (27)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingОт EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingРейтинг: 4 из 5 звезд4/5 (1138)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeОт EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeРейтинг: 4.5 из 5 звезд4.5/5 (253)