Вам также может понравиться
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Export As TextДокумент1 страницаExport As Textetruelia50Оценок пока нет
- Sign A PDFДокумент1 страницаSign A PDFetruelia50Оценок пока нет
- LicenseДокумент7 страницLicenseetruelia50Оценок пока нет
- Page Setup... Zoom in Zoom Out Print... Hide MarginsДокумент1 страницаPage Setup... Zoom in Zoom Out Print... Hide Marginsetruelia50Оценок пока нет
- ReadmeДокумент1 страницаReadmeetruelia50Оценок пока нет
- View Object MetadataДокумент1 страницаView Object Metadataetruelia50Оценок пока нет
- Select and Copy An ImageДокумент1 страницаSelect and Copy An Imageetruelia50Оценок пока нет
- Validate SignaturesДокумент1 страницаValidate Signaturesetruelia50Оценок пока нет
- Indicate Final Approval: Related InformationДокумент1 страницаIndicate Final Approval: Related Informationetruelia50Оценок пока нет
- Change How A Comment Appears: Related InformationДокумент1 страницаChange How A Comment Appears: Related Informationetruelia50Оценок пока нет
- Select and Copy TextДокумент1 страницаSelect and Copy Textetruelia50Оценок пока нет
- Reader En-Us Report-DuplicateДокумент1 страницаReader En-Us Report-Duplicateetruelia50Оценок пока нет
- VersionДокумент1 страницаVersionetruelia50Оценок пока нет
- Reader En-Us Report-ContentДокумент21 страницаReader En-Us Report-Contentetruelia50Оценок пока нет
- Reader En-Us Report-SummaryДокумент2 страницыReader En-Us Report-Summaryetruelia50Оценок пока нет
- Print A BookletДокумент1 страницаPrint A Bookletetruelia50Оценок пока нет
- Add SecurityДокумент1 страницаAdd Securityetruelia50Оценок пока нет
- Reader En-Us Report-IndexesДокумент1 страницаReader En-Us Report-Indexesetruelia50Оценок пока нет
- Reader En-Us Report-XrefДокумент8 страницReader En-Us Report-Xrefetruelia50Оценок пока нет
- Link ErrorДокумент1 страницаLink Erroretruelia50Оценок пока нет
- Install 2Документ1 страницаInstall 2etruelia50Оценок пока нет
- Reader En-Us Report-ImageДокумент2 страницыReader En-Us Report-Imageetruelia50Оценок пока нет
- WelcomeДокумент1 страницаWelcomeetruelia50Оценок пока нет
- This Topic Is in The Help System of Another Product. To View The Topic, Install That ProductДокумент1 страницаThis Topic Is in The Help System of Another Product. To View The Topic, Install That Productanon-4445Оценок пока нет
- ToobusyДокумент1 страницаToobusyetruelia50Оценок пока нет
- UsernameДокумент1 страницаUsernameetruelia50Оценок пока нет
- RpberrДокумент1 страницаRpberretruelia50Оценок пока нет
- ScntlastДокумент1 страницаScntlastetruelia50Оценок пока нет
- SecurityДокумент1 страницаSecurityetruelia50Оценок пока нет
- TimezoneДокумент1 страницаTimezoneetruelia50Оценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- News WritingДокумент2 страницыNews Writingpheonixmtbt100% (3)
- 2-A Phasing of Full Assumption of Devolved Functions For PCMs (Annex F-1)Документ3 страницы2-A Phasing of Full Assumption of Devolved Functions For PCMs (Annex F-1)Michelle Gozon60% (5)
- GO Ms 874 PDFДокумент15 страницGO Ms 874 PDFAnupoju Appalaraju0% (1)
- Job Profile Chart l4&5-16112011Документ3 страницыJob Profile Chart l4&5-16112011syahrainamir100% (1)
- Residency ProgramsДокумент72 страницыResidency Programsmorasaki003Оценок пока нет
- AstraZeneca AB v. Sun Pharma Global FZE Et. Al.Документ14 страницAstraZeneca AB v. Sun Pharma Global FZE Et. Al.PriorSmartОценок пока нет
- Burj Al Arab HseДокумент2 страницыBurj Al Arab HseLedo HoussienОценок пока нет
- Kimberley Hoff PAR 115 Portfolio #8Документ3 страницыKimberley Hoff PAR 115 Portfolio #8legalparaeagleОценок пока нет
- Excecutive Summary - US CovidДокумент125 страницExcecutive Summary - US CovidDiego CorreaОценок пока нет
- As en 12182-2002 Technical Aids For Disabled Persons - General Requirements and Test MethodsДокумент8 страницAs en 12182-2002 Technical Aids For Disabled Persons - General Requirements and Test MethodsSAI Global - APACОценок пока нет
- Radio OperatorДокумент2 страницыRadio OperatorStefanОценок пока нет
- Pharmaceutical and Food Safety Bureau, Ministry of Health, Labour and Welfare Translated by Office of Safety I, Pharmaceuticals and Medical Devices AgencyДокумент19 страницPharmaceutical and Food Safety Bureau, Ministry of Health, Labour and Welfare Translated by Office of Safety I, Pharmaceuticals and Medical Devices Agencyعبدالعزيز بدرОценок пока нет
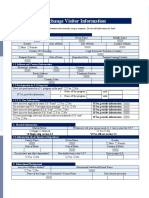
- Exchange Visitor InformationДокумент3 страницыExchange Visitor InformationPrathamesh ParabОценок пока нет
- Memorandum To Benard Berelson 1969-EUGENISME PREUVEДокумент1 страницаMemorandum To Benard Berelson 1969-EUGENISME PREUVEcruxsacraОценок пока нет
- The Role of Safety OfficerДокумент10 страницThe Role of Safety OfficerSiddharth100% (1)
- AD9 Go-CommunityEvac Center ProposalДокумент25 страницAD9 Go-CommunityEvac Center ProposalDanielle Go100% (1)
- The Daily Tar Heel For April 1, 2013Документ13 страницThe Daily Tar Heel For April 1, 2013The Daily Tar Heel100% (1)
- World Health OrganizationДокумент17 страницWorld Health OrganizationRichi SinghОценок пока нет
- My Sister Killed On Her Mission by The Mission President's Wife in Portland - Exmormon PDFДокумент64 страницыMy Sister Killed On Her Mission by The Mission President's Wife in Portland - Exmormon PDFMatthew Rivera100% (1)
- Visum UnterlagenДокумент19 страницVisum Unterlagenapi-289435089Оценок пока нет
- Good Home Pet Adoptions, Inc. Cat Foster Home AgreementДокумент6 страницGood Home Pet Adoptions, Inc. Cat Foster Home AgreementJustin CollierОценок пока нет
- MediamintДокумент1 страницаMediamintKaparthi GujjarОценок пока нет
- AIPGMEE 2016 - Book Recent PDFДокумент72 страницыAIPGMEE 2016 - Book Recent PDFdorjeesengeОценок пока нет
- Schedule 1 For 2019 Form 1040Документ1 страницаSchedule 1 For 2019 Form 1040CNBC.comОценок пока нет
- Mike PenceДокумент50 страницMike PencepersonstakeplaceОценок пока нет
- WorldInequalityLab Issue Brief 2021.01 CovidДокумент18 страницWorldInequalityLab Issue Brief 2021.01 CovidKepa NeritaОценок пока нет
- Census VPMДокумент14 страницCensus VPMRavi ChandranОценок пока нет
- Greenleaf RhodeIslandDOCSДокумент95 страницGreenleaf RhodeIslandDOCSTimothy TuckОценок пока нет
- Social Town Planning FrontsДокумент17 страницSocial Town Planning FrontsGappmaauОценок пока нет
- Engleski - Šalić 1Документ19 страницEngleski - Šalić 1Leonarda PavićОценок пока нет