Вам также может понравиться
- Great Eastern Life - Confidential Medical Certificate (Stroke) - CLMLAMCSДокумент2 страницыGreat Eastern Life - Confidential Medical Certificate (Stroke) - CLMLAMCSsimpoonОценок пока нет
- Prulife Uk Form PiДокумент3 страницыPrulife Uk Form PiPaulie TitoОценок пока нет
- Attending Physicians Statement Crisis Cover Muscular Dystrophy - 041222Документ2 страницыAttending Physicians Statement Crisis Cover Muscular Dystrophy - 041222laraОценок пока нет
- Ti Claim FormДокумент8 страницTi Claim FormHihiОценок пока нет
- Great Eastern Life - Confidential Medical Certificate (Other Illnesses) - CLMLAMCOДокумент2 страницыGreat Eastern Life - Confidential Medical Certificate (Other Illnesses) - CLMLAMCOsimpoonОценок пока нет
- CC Stroke NewДокумент12 страницCC Stroke NewHihiОценок пока нет
- Physician Statement for Life InsuranceДокумент2 страницыPhysician Statement for Life InsuranceJake CopradeОценок пока нет
- Crisis Care Accelerator ClaimДокумент9 страницCrisis Care Accelerator ClaimHihiОценок пока нет
- Family FLoater FormДокумент6 страницFamily FLoater FormSantosh KodereОценок пока нет
- PM OthersДокумент35 страницPM OthersHihiОценок пока нет
- ZLIMB Life Claim Questionnaire FormДокумент2 страницыZLIMB Life Claim Questionnaire FormAdyna MynameОценок пока нет
- Attending Physicians Statement Crisis Cover Major Organ Transplant - 041222Документ2 страницыAttending Physicians Statement Crisis Cover Major Organ Transplant - 041222max leeОценок пока нет
- Beneficial Life Insurance FormДокумент1 страницаBeneficial Life Insurance FormRanieza CastilloОценок пока нет
- S10.1 General Med Request - AutomatedДокумент5 страницS10.1 General Med Request - AutomatedSuresh LukoseОценок пока нет
- Crisis Cover Claim Form GuideДокумент13 страницCrisis Cover Claim Form GuideHihiОценок пока нет
- Claim Form GeneralДокумент1 страницаClaim Form GeneralTanya Rose-AppleОценок пока нет
- AIA Singapore Death Claim FormДокумент3 страницыAIA Singapore Death Claim FormPunaОценок пока нет
- PP CformДокумент4 страницыPP CformHihiОценок пока нет
- DGH(2)Документ2 страницыDGH(2)ranju ramachandranОценок пока нет
- Attending Physicians Statement Crisis Cover Renal Failure - 041222Документ2 страницыAttending Physicians Statement Crisis Cover Renal Failure - 041222max leeОценок пока нет
- 680 DGHДокумент4 страницы680 DGHjdchandrapal4980Оценок пока нет
- Proposal Form For New India Premier MediclaimДокумент6 страницProposal Form For New India Premier MediclaimAnonymous 95dlTK1McОценок пока нет
- HSBC Death Claim FormДокумент5 страницHSBC Death Claim Form健康生活園Healthy Life GardenОценок пока нет
- Proposal Form New India Mediclaim Policy 01102021Документ6 страницProposal Form New India Mediclaim Policy 01102021abcdefabcОценок пока нет
- Proposal Form New India Mediclaim PolicyДокумент6 страницProposal Form New India Mediclaim PolicyPavan Kumar NarbolikarОценок пока нет
- Confidential Medical Certificate (Total and Permanent Disability) PDFДокумент3 страницыConfidential Medical Certificate (Total and Permanent Disability) PDFJP PalamОценок пока нет
- Crisis Cover Kids Claim Form SummaryДокумент16 страницCrisis Cover Kids Claim Form SummaryHihiОценок пока нет
- Proposal Form New India Floater Mediclaim Policy 21012020 - 1Документ6 страницProposal Form New India Floater Mediclaim Policy 21012020 - 1aj iseОценок пока нет
- FB ClaimДокумент14 страницFB ClaimHihiОценок пока нет
- Hospitalization Reimbursment Claim FormДокумент4 страницыHospitalization Reimbursment Claim FormFarhan aliОценок пока нет
- Medical Benefit and Hospital & Surgical Claim Form - Claimant'S StatementДокумент7 страницMedical Benefit and Hospital & Surgical Claim Form - Claimant'S StatementatzharОценок пока нет
- Attending Physicians StatementДокумент2 страницыAttending Physicians StatementDionie Wilson DiestroОценок пока нет
- Proposal Form New India Floater Mediclaim Policy-1Документ7 страницProposal Form New India Floater Mediclaim Policy-1Hemraj SonarОценок пока нет
- Claim - Form - MediassitДокумент4 страницыClaim - Form - MediassitKashish BangaloreОценок пока нет
- NTUC Pa Paid Claim Form (08 2017)Документ5 страницNTUC Pa Paid Claim Form (08 2017)pat5355Оценок пока нет
- Kutumb Swasthya Bima Policy - GroupДокумент4 страницыKutumb Swasthya Bima Policy - Grouprohit kakkarОценок пока нет
- Medical Report and ReceiptДокумент5 страницMedical Report and Receiptkumarsam087Оценок пока нет
- Revival FormДокумент3 страницыRevival Formpradheepkr50Оценок пока нет
- MET - Medical Claim Reimbursement Form in Patient - KWTДокумент2 страницыMET - Medical Claim Reimbursement Form in Patient - KWTangeloriondo1217Оценок пока нет
- F. NO. 680 (Rev.2022) Date of Receipt Inward No.Документ2 страницыF. NO. 680 (Rev.2022) Date of Receipt Inward No.Ram Shanker DewanganОценок пока нет
- Lonpac Maid Medical ClaimДокумент3 страницыLonpac Maid Medical ClaimYl EdianonОценок пока нет
- Surat Keterangan Dokter - Doctor'S Report Penyakit Kanker - CancerДокумент5 страницSurat Keterangan Dokter - Doctor'S Report Penyakit Kanker - CancerUlinnoha FarrasОценок пока нет
- Personal Accident Critical Illness Hospital Income Claim FormДокумент3 страницыPersonal Accident Critical Illness Hospital Income Claim FormHihiОценок пока нет
- FB Pregnancy-ComplicationДокумент19 страницFB Pregnancy-ComplicationHihiОценок пока нет
- Medical Examiner'S Confidential ReportДокумент2 страницыMedical Examiner'S Confidential ReportParesh BorboruahОценок пока нет
- Claims - Death Claim FormДокумент6 страницClaims - Death Claim Formwaran RMОценок пока нет
- Great EasternДокумент2 страницыGreat EasternWeng Meng VISTAОценок пока нет
- Death Claim Checklist 2017Документ4 страницыDeath Claim Checklist 2017Cheche GonzalesОценок пока нет
- Claim Form IPD FormatДокумент2 страницыClaim Form IPD FormataccsaanvibajajОценок пока нет
- Generi Life Physician Statement FormДокумент1 страницаGeneri Life Physician Statement FormVennus RacraquinОценок пока нет
- CLAIM FORM SUBMISSION GUIDEДокумент1 страницаCLAIM FORM SUBMISSION GUIDEAnonymous W9VINoTza100% (1)
- Declaration of Good Health Form - With Covid QДокумент2 страницыDeclaration of Good Health Form - With Covid QRajnish YadavОценок пока нет
- Aon - Aia Ghs Claim Form - Oct 2014Документ3 страницыAon - Aia Ghs Claim Form - Oct 2014John SmithОценок пока нет
- Proposal Form Ashakiran PDFДокумент6 страницProposal Form Ashakiran PDFSreejith Rajendran PillaiОценок пока нет
- OMP Proposal Form (Business and Holiday) PDFДокумент6 страницOMP Proposal Form (Business and Holiday) PDFdhananjay shuklaОценок пока нет
- AXA Hypertension QuestionnaireДокумент2 страницыAXA Hypertension QuestionnaireClaudine Limasa TabudlongОценок пока нет
- 50 English Essay PracticeДокумент1 страница50 English Essay PracticesiewharОценок пока нет
- Great Eastern Life - Living Assurance Claim Form-Personal Statement - LACFPSДокумент4 страницыGreat Eastern Life - Living Assurance Claim Form-Personal Statement - LACFPSsimpoonОценок пока нет
- Your Bones Are Living Tissue and Always Changing. They Not Only Support Your Body But Also Serve As A Depository For Important MineralsДокумент30 страницYour Bones Are Living Tissue and Always Changing. They Not Only Support Your Body But Also Serve As A Depository For Important Mineralssimpoon100% (1)
- This Enlargement of A Lung Segment Shows Bronchioles and Alveoli. The Alveoli Exchange Oxygen and Carbon Dioxide Between The Air and Your BloodДокумент15 страницThis Enlargement of A Lung Segment Shows Bronchioles and Alveoli. The Alveoli Exchange Oxygen and Carbon Dioxide Between The Air and Your BloodsimpoonОценок пока нет
- London & Pacific Insurance - HouseownerДокумент8 страницLondon & Pacific Insurance - HouseownersimpoonОценок пока нет
- TAKAFUL IKLAS Hospital Is at Ion Claim FormДокумент2 страницыTAKAFUL IKLAS Hospital Is at Ion Claim FormsimpoonОценок пока нет
- London & Pacific Insurance - FireДокумент10 страницLondon & Pacific Insurance - FiresimpoonОценок пока нет
- London & Pacific Insurance - ConlossДокумент6 страницLondon & Pacific Insurance - Conlosssimpoon100% (1)
- TAKAFUL IKLAS - Attending Physician Statement TPD PPDДокумент3 страницыTAKAFUL IKLAS - Attending Physician Statement TPD PPDsimpoonОценок пока нет
- TAKAFUL IKLAS Motor Wind Screen Claim FormДокумент2 страницыTAKAFUL IKLAS Motor Wind Screen Claim FormsimpoonОценок пока нет
- Great Eastern Life - Notification of Death Claim - NODCДокумент2 страницыGreat Eastern Life - Notification of Death Claim - NODCsimpoonОценок пока нет
- TAKAFUL IKLAS Critical Illness Claim FormДокумент2 страницыTAKAFUL IKLAS Critical Illness Claim FormsimpoonОценок пока нет
- TAKAFUL IKLAS Personal Accident (PA) ClaimДокумент4 страницыTAKAFUL IKLAS Personal Accident (PA) ClaimsimpoonОценок пока нет
- TAKAFUL IKLAS Claims Release FormДокумент1 страницаTAKAFUL IKLAS Claims Release FormsimpoonОценок пока нет
- TAKAFUL IKLAS - Attending Physician Statement (Death)Документ2 страницыTAKAFUL IKLAS - Attending Physician Statement (Death)simpoonОценок пока нет
- Great Eastern Life - DoctorstatementДокумент4 страницыGreat Eastern Life - DoctorstatementsimpoonОценок пока нет
- TAKAFUL IKLAS Motor Accident Report FormДокумент4 страницыTAKAFUL IKLAS Motor Accident Report FormsimpoonОценок пока нет
- Great Eastern Life - Letter of Author Is at Ion Consent - LOAC (1) 1Документ2 страницыGreat Eastern Life - Letter of Author Is at Ion Consent - LOAC (1) 1simpoonОценок пока нет
- Great Eastern Life - Authorisation To Collect Claim(s) Payment Cheque(s) - ATCДокумент2 страницыGreat Eastern Life - Authorisation To Collect Claim(s) Payment Cheque(s) - ATCsimpoonОценок пока нет
- Great Eastern Life - Letter of AuthorisationConsent - LOAC (2) 1Документ2 страницыGreat Eastern Life - Letter of AuthorisationConsent - LOAC (2) 1simpoonОценок пока нет
- Great Eastern Life - Letter of Author Is at Ion Consent - LOACДокумент2 страницыGreat Eastern Life - Letter of Author Is at Ion Consent - LOACsimpoonОценок пока нет
- Great Eastern Life - deathClaimFormДокумент4 страницыGreat Eastern Life - deathClaimFormsimpoonОценок пока нет
- Great Eastern Life - Confidential Medical Certificate (Heart AttackCoronory Artery By-Pass Surgery) - CLMLAMHCДокумент2 страницыGreat Eastern Life - Confidential Medical Certificate (Heart AttackCoronory Artery By-Pass Surgery) - CLMLAMHCsimpoonОценок пока нет
- Great Eastern Life - Accident Claim Form To Be Completed by Assured Claimant - ACF (LA)Документ4 страницыGreat Eastern Life - Accident Claim Form To Be Completed by Assured Claimant - ACF (LA)simpoonОценок пока нет
- Great Eastern Life - Accident Claim Form Attending Physician's Statement - ACF (PS)Документ4 страницыGreat Eastern Life - Accident Claim Form Attending Physician's Statement - ACF (PS)simpoonОценок пока нет
- Great Eastern Life - Panel of Hospital - HospitalListv23 - 042007Документ2 страницыGreat Eastern Life - Panel of Hospital - HospitalListv23 - 042007simpoon100% (1)
- Adolf Erman Life in Ancient EgyptДокумент618 страницAdolf Erman Life in Ancient EgyptRCEBОценок пока нет
- Choose The Best AnswersДокумент5 страницChoose The Best Answersnguyen Thanh PhuongОценок пока нет
- Service Manual Sigma Air Control Plus: Article Number: 7.7740.0 7.7741.0 7.7742.0Документ47 страницService Manual Sigma Air Control Plus: Article Number: 7.7740.0 7.7741.0 7.7742.0Evandro Jva compressoresОценок пока нет
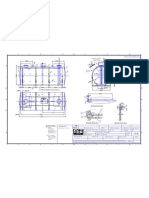
- Saddle Positioning (500m3)Документ1 страницаSaddle Positioning (500m3)solquihaОценок пока нет
- Problems On Fluid PropertiesДокумент1 страницаProblems On Fluid PropertiesErvenjee BascoОценок пока нет
- 793D Machine SystemДокумент52 страницы793D Machine SystemWillington Augusto Ariza100% (5)
- Forming OriginalДокумент16 страницForming OriginalJulio QuitoОценок пока нет
- New Microsoft Office Word DocumentДокумент6 страницNew Microsoft Office Word Documentkhengarsadiya99Оценок пока нет
- Master Your TimeДокумент55 страницMaster Your TimeRobinvarshneyОценок пока нет
- IPasolink EX Full Outdoor 70 80GHzДокумент2 страницыIPasolink EX Full Outdoor 70 80GHzIbrahim MaihoubОценок пока нет
- MATERIAL SAFETY DATA SHEET FOR DEVELOPER D-78Документ4 страницыMATERIAL SAFETY DATA SHEET FOR DEVELOPER D-78Bachrul UlumОценок пока нет
- Nguyên Lý MARKETINGДокумент22 страницыNguyên Lý MARKETINGThảo An TrịnhОценок пока нет
- Activity in 21st Century LiteratureДокумент3 страницыActivity in 21st Century Literatureheart AquinoОценок пока нет
- SINHGAD COLLEGE SPECIFICATION WRITING EXAM QUESTION BANKДокумент2 страницыSINHGAD COLLEGE SPECIFICATION WRITING EXAM QUESTION BANKshaolinОценок пока нет
- Género y Literatura en Los Países de Habla InglesaДокумент24 страницыGénero y Literatura en Los Países de Habla InglesaLuis Arevalo100% (1)
- WibreeДокумент17 страницWibreeSagar Acharya100% (1)
- Public Environmental and Social Data SheetДокумент2 страницыPublic Environmental and Social Data SheetOLD TV5Оценок пока нет
- Exploring Business Operations at OM LogisticsДокумент66 страницExploring Business Operations at OM LogisticsGundeep SinGhОценок пока нет
- Osf Unit 3 PDFДокумент16 страницOsf Unit 3 PDFRaRaRaОценок пока нет
- Ghosts Through HistoryДокумент11 страницGhosts Through HistoryKhianna JohnsonОценок пока нет
- The Secret of Khechari MudraДокумент5 страницThe Secret of Khechari MudraPhalgun Balaaji100% (2)
- Servo Amplifier Mr-j2s - AДокумент323 страницыServo Amplifier Mr-j2s - AGeuris David Estèvez BelliardОценок пока нет
- Class 9-WS-sci-II Chapter. 18Документ3 страницыClass 9-WS-sci-II Chapter. 18ddddОценок пока нет
- SC Drivers & MetricsДокумент27 страницSC Drivers & MetricsHaris KhanОценок пока нет
- IntraOs 70 UNV Version 5.03 SERVICEДокумент56 страницIntraOs 70 UNV Version 5.03 SERVICEJosé RivasОценок пока нет
- All Charts From The Brain Over Binge Recovery GuideДокумент13 страницAll Charts From The Brain Over Binge Recovery GuideLupita Mora LobacoОценок пока нет
- UG - PG Lab EquipmentsДокумент117 страницUG - PG Lab EquipmentssrajeceОценок пока нет
- Oliver Heaviside Physical MathematicianДокумент7 страницOliver Heaviside Physical MathematicianAKHI9Оценок пока нет
- Thrive Strongman ProgramДокумент6 страницThrive Strongman Programahmed z falahОценок пока нет
- Manual MICOM P220 MotoresДокумент410 страницManual MICOM P220 MotoresGustavo TrilloОценок пока нет