Date 12/17/2009 IDAHO DEPARTMENT OF HEALTH AND WELFARE CHILD AND FAMILY SERVICES
PART A - SAFETY ASSESSMENT
Referral Date: Region: Priority: Date Child Seen: Family Name: Worker Name: Presenting Issue #: Time Child Seen: Family ID: Worker ID: Assessment ID:
Instructions: Complete this form within 30 days after first seeing the child.
CPS History Review (FCSIS & FOCUS) Safety Summary Narrative: Worker: Date:
( ) Family has prior referrals
Time:
SECTION 1: SAFETY ASSESSMENT
Directions: The following factors are behaviors or conditions that may be associated with safety threats to a child(ren). These threats involve both present and emerging danger. This assessment will include all children in the family who are identified as being at risk. Consider the effects that adults who have access to them could have on their safety. Identify each factor by checking 'yes' when the information currently available indicates a clear presence of the safety factor, 'No' when the information currently available does not indicate presence of the safety factor, or 'Inconclusive' when the information currently available is insufficient or contradictory.
# 1 2
Yes
No
Incon.
Question Caregiver or alleged offender's behavior is violent and/or out of control. Caregiver or alleged offender describes or acts toward child in predominantly negative terms or has extremely unrealistic expectations given the child's age or level of development. Comment: Caregiver or alleged offender causes harm or has made a plausible threat of harm to the child. Child is fearful of people living in or frequenting the home. Child sexual abuse is suspected and circumstances suggest that there may be immediate risk of harm to child. Caregiver or alleged offender has not, will not, or cannot provide sufficient supervision to protect child from immediate risk of harm. Comment: Death of a sibling or other child in the household has ever occurred due to abuse/neglect or uncertain circumstances.
3 4 5 6
SAFETY ASSESSMENT
8 9 10 11
Caregiver or alleged offender had parental rights terminated previously due to abuse or neglect. Child has positive toxicology from drugs or alcohol. Alleged offender may have previously abused/neglected this child/children and now has unrestricted access to child. The current alleged abuse or neglect is severe and suggests that there may be immediate and urgent risk to the child. Comment: Caregiver or alleged offender's alleged or observed drug or alcohol use may seriously affect his/her ability to supervise, protect, or care for the child. Caregiver or alleged offender may be a victim of family violence which affects caretaker's ability to care for and/or protect child from immediate harm. There is a pattern of escalating severity of harm. Comment: Child's whereabouts cannot be ascertained and/or there is reason to believe that the family is about to flee or refuses access to the child. Comment: Caregiver or alleged offender has not or is unable to meet the child's immediate needs for food, clothing, shelter, and/or medical care; the child's physical living conditions are hazardous and may cause harm. Comment: Caregiver, alleged offender, or child has a severe and/or chronic mental or physical illness or disability and current supports are not in place to ensure child safety. Other risk of immediate harm (specify in comment area).
12 13 14 15
16
17 18
Child Characteristics
# 1 2 3 4 Vulnerability/Lack of Self-Protection Skills/Special Needs. Comment: Behavior Problems. Comment: Previously been placed outside the home. Comment: Other (specify in comment area). Comment: Collaterals
Yes
No
Incon.
SAFETY ASSESSMENT
SECTION 2: SAFETY DECISION
Directions: Identify your safety decision by checking the appropriate box below. (You may check more than one box if different safety decisions apply to different children.) This decision should be based on the assessment of all threats of present or emerging danger and any other information known about this case
() () ()
A. Safe: B. Conditionally Safe: C. Unsafe:
There are no threats of present or emerging danger that could cause the child(ren) to be seriously harmed. A plan is being implemented to resolve the safety threats identified at the present time. One or more child(ren) is in imminent danger (requires placement)
SECTION 3: IMMEDIATE PROTECTION/SAFETY PLAN
Describe the immediate protection plan as follows: - what actions have or will be taken to protect each child in relation to current threats of present or emerging danger : and - who is responsible for implementing each plan component: and - how the plan will be monitored and by whom - address the role of family strengths (including extended family) and mitigating circumstances in the plan - address services and/or adaptive supports that could be put in place to assist a family member who has a disability Safety Plan Narrative:
Worker:
Date:
Time: Yes ( ) No ( ) If 'No' explain, if 'Yes' provide the date:
Was the interview with the child taped? Comment: Has the referring party been recontacted? Comment:
Yes ( )
No ( ) If 'No' explain, if 'Yes' provide the date:
If there is no court action, is the family willing to participate in a voluntary service plan?
Yes ( ) No ( ) N/A ( )
SAFETY ASSESSMENT
48 Hour Review for Children Ages 6 and Under:
SECTION 4: ASSESSMENT DECISION, CASE STATUS, AND DISPOSITIONAL STATEMENT
CASE STATUS (check one) ( ) Case remains open ( ) Case closed with supervisory approval ( ) Unable to locate family
PART B COMPREHENSIVE ASSESSMENT SHALL BE COMPLETED WHEN SAFETY THREATS ARE IDENTIFIED, AND THE CASE REMAINS OPEN FOR SERVICES: DISPOSITIONAL STATEMENT IS NOT REQUIRED IF A PART B COMPREHENSIVE ASSESSMENT WILL BE COMPLETED
Dispositional Statement If Substantiated, Date Notification letter sent: Child Name Suspect Name Reason Date Disposition Rmvd Frm Cntrl Reg
Disposition Narrative:
SECTION 5: SIGNATURES/DATES
Safety Assessment Review Due Date: Staff: Date:
Worker: _______________________________________________________ Date: ______________________________ Supervisor: _____________________________________________________ Date: ______________________________
SAFETY ASSESSMENT
Вам также может понравиться
- Hawaii Child Safety Assessment 3 11Документ5 страницHawaii Child Safety Assessment 3 11Rick ThomaОценок пока нет
- Hawaii FSS VCM Child Safety Assessment Instructions 3 11Документ2 страницыHawaii FSS VCM Child Safety Assessment Instructions 3 11Rick ThomaОценок пока нет
- Louisiana Safety Assessment 10-17-2011Документ2 страницыLouisiana Safety Assessment 10-17-2011Rick ThomaОценок пока нет
- West Virginia CPS - Family Functioning Assessment - Rev 2012Документ7 страницWest Virginia CPS - Family Functioning Assessment - Rev 2012Rick ThomaОценок пока нет
- Hawaii Child Safety Assessment and in Home Safety Plan Instructions 3 11Документ7 страницHawaii Child Safety Assessment and in Home Safety Plan Instructions 3 11Rick ThomaОценок пока нет
- Immediate Safety AssessmentДокумент3 страницыImmediate Safety AssessmentIrene JordanОценок пока нет
- Hawaii Safety of Placement Assessment 3 11Документ3 страницыHawaii Safety of Placement Assessment 3 11Rick ThomaОценок пока нет
- New Mexico CYFD - Safety Assessment - Rev 2010Документ6 страницNew Mexico CYFD - Safety Assessment - Rev 2010Rick ThomaОценок пока нет
- Louisiana SDM Screening and Response Assessment 10-17-2011Документ22 страницыLouisiana SDM Screening and Response Assessment 10-17-2011Rick ThomaОценок пока нет
- ABE Protocol Jan 2016Документ5 страницABE Protocol Jan 2016Romina LeivaОценок пока нет
- Ahs8100 SDM Intake TemplateДокумент6 страницAhs8100 SDM Intake Templateapi-277510691Оценок пока нет
- Cps Pregnancy GuidelinesДокумент10 страницCps Pregnancy GuidelinesCece MОценок пока нет
- CHCPRT001 - R-L ANDERSON Assessment Task 5 PortfolioДокумент4 страницыCHCPRT001 - R-L ANDERSON Assessment Task 5 PortfolioAndrea AndersonОценок пока нет
- Case Management Manager JDДокумент11 страницCase Management Manager JDPeace Children أطفال السلامОценок пока нет
- Workbook and Assessment Record v01Документ12 страницWorkbook and Assessment Record v01MyGTMOAngel2009Оценок пока нет
- West Virginia CPS - Present Danger Assessment - Risk Assessment ToolДокумент5 страницWest Virginia CPS - Present Danger Assessment - Risk Assessment ToolRick ThomaОценок пока нет
- Colorado CPS - Family Risk Assessment - InstructionsДокумент12 страницColorado CPS - Family Risk Assessment - InstructionsRick ThomaОценок пока нет
- Mandatory Report FormДокумент2 страницыMandatory Report Formapi-297340865Оценок пока нет
- Starting A Childcare Business - Guide To Setting Up A Childcare CenterОт EverandStarting A Childcare Business - Guide To Setting Up A Childcare CenterОценок пока нет
- Tesi CДокумент14 страницTesi CKatrina Katrina100% (1)
- DSS Safety PlanДокумент2 страницыDSS Safety PlanMyrtleBeachSC newsОценок пока нет
- Floridas DepesДокумент21 страницаFloridas DepesGabriel Vidal SandovalОценок пока нет
- 0511B FPO RiskAssessmentDefinitionsДокумент6 страниц0511B FPO RiskAssessmentDefinitionsCatarina FonsecaОценок пока нет
- Child Safeguarding Policy and Procedure VДокумент13 страницChild Safeguarding Policy and Procedure Vapi-240127110Оценок пока нет
- Assessment GuidanceДокумент46 страницAssessment GuidancetiggieОценок пока нет
- EarlyChildhood ReportingTemplateДокумент12 страницEarlyChildhood ReportingTemplateryansingla13Оценок пока нет
- Eo Cic Child Safeguarding Policy and ProcedureДокумент12 страницEo Cic Child Safeguarding Policy and Procedureapi-240127110Оценок пока нет
- 3 13 Child Abuse and NeglectДокумент18 страниц3 13 Child Abuse and Neglectapi-259168827Оценок пока нет
- Child 20protection 20policy BB 2012Документ27 страницChild 20protection 20policy BB 2012imaan0% (1)
- 2014 Child Protection - 2nd LevelДокумент35 страниц2014 Child Protection - 2nd Levelapi-297389221Оценок пока нет
- Mandatory Reporting PolicyДокумент6 страницMandatory Reporting Policyapi-319586327Оценок пока нет
- Child Protection Case ConferencesДокумент3 страницыChild Protection Case ConferencesKenneth BarnesОценок пока нет
- Children's Medication Toolbox: Managing, Monitoring and Improving Your Child's Response to MedicationОт EverandChildren's Medication Toolbox: Managing, Monitoring and Improving Your Child's Response to MedicationОценок пока нет
- Safeguarding Children-Child ProtectionДокумент5 страницSafeguarding Children-Child ProtectionKingsland Pre-SchoolОценок пока нет
- Child Protection Policy: Blue Bay Early Learning CentreДокумент6 страницChild Protection Policy: Blue Bay Early Learning CentreAnna-Louise Belle0% (1)
- Child Protection Policy: PART A: The Care and Protection ActДокумент13 страницChild Protection Policy: PART A: The Care and Protection ActjacafyОценок пока нет
- Neglect and AttachmentДокумент27 страницNeglect and AttachmentMaximMadalinaIulianaОценок пока нет
- The Common Assessment Framework For Children & Young People: Supporting ToolsДокумент32 страницыThe Common Assessment Framework For Children & Young People: Supporting ToolsSarah SmithОценок пока нет
- Vulnerable Victims Policy2Документ4 страницыVulnerable Victims Policy2quietvolcanoОценок пока нет
- Seen But Not Heard Investigative Report 2019Документ28 страницSeen But Not Heard Investigative Report 2019Jenn HoeggОценок пока нет
- Child Protection Policy AppendicesДокумент10 страницChild Protection Policy AppendicesdickovskiОценок пока нет
- Unit 2: Webquest: Factors To Help Build Child ResiliencyДокумент4 страницыUnit 2: Webquest: Factors To Help Build Child Resiliencyapi-549321789Оценок пока нет
- Tittle 22Документ3 страницыTittle 22api-220884896Оценок пока нет
- Relevance of Child Protection Across All Health AnДокумент7 страницRelevance of Child Protection Across All Health AnTitser Jr Kagura MainОценок пока нет
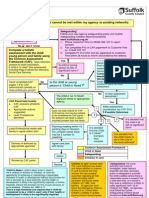
- Integrated Assessment Model SuffolkДокумент2 страницыIntegrated Assessment Model SuffolkGinaAlexaCîmpianuОценок пока нет
- 10 5 Child Abuse and Neglect Example PolicyДокумент2 страницы10 5 Child Abuse and Neglect Example Policytop writerОценок пока нет
- Hawaii Risk Assessment Rating Tool Instructions and Overview 3 11Документ4 страницыHawaii Risk Assessment Rating Tool Instructions and Overview 3 11Rick ThomaОценок пока нет
- Profiling and Initial Risk Assessment Tools For Children-at-RiskДокумент6 страницProfiling and Initial Risk Assessment Tools For Children-at-RiskGEGAYОценок пока нет
- Duty To ReportДокумент3 страницыDuty To ReportJeffrey FawcettОценок пока нет
- In-Service Lesson Plan Mandated Reporting in The Education System 1Документ20 страницIn-Service Lesson Plan Mandated Reporting in The Education System 1api-549169454Оценок пока нет
- 1227-S2.e SBR WM Oc 21Документ7 страниц1227-S2.e SBR WM Oc 21kandycxane87Оценок пока нет
- Sas 21Документ2 страницыSas 21Gwenn SalazarОценок пока нет
- Corona-Norco Unified School District's Employee Handbook of Mandated Notifications 2023-2024, Pages 6-12Документ7 страницCorona-Norco Unified School District's Employee Handbook of Mandated Notifications 2023-2024, Pages 6-12The Press-Enterprise / pressenterprise.comОценок пока нет
- b23 Eval - AssesguidanceДокумент11 страницb23 Eval - AssesguidanceKaren ClarkОценок пока нет
- Child Protection PolicyДокумент18 страницChild Protection PolicyscoilchillruadhainОценок пока нет
- R & C of Sexual Activity: Lesson 6, Analysis of Recent Developments in Repro HealthДокумент3 страницыR & C of Sexual Activity: Lesson 6, Analysis of Recent Developments in Repro Healthkelmg97Оценок пока нет
- 1622728693child ProtectionДокумент12 страниц1622728693child ProtectionPhyu Sin WinОценок пока нет
- Nar Nar Goon Primary School: Mandatory Reporting PolicyДокумент5 страницNar Nar Goon Primary School: Mandatory Reporting Policyapi-419396853Оценок пока нет
- Tinsley V Flanagan AZ DES Class Action Complaint 2015Документ51 страницаTinsley V Flanagan AZ DES Class Action Complaint 2015Rick Thoma0% (1)
- Orange County Grand Jury Fostering A Better Foster Care System 2016Документ38 страницOrange County Grand Jury Fostering A Better Foster Care System 2016Rick Thoma0% (1)
- Comments On The Five Year Anniversary of The Administration For Children's ServicesДокумент21 страницаComments On The Five Year Anniversary of The Administration For Children's ServicesRick ThomaОценок пока нет
- Justice Denied: The Crisis in Legal Representation of Birth Parents in Child Protective ProceedingsДокумент77 страницJustice Denied: The Crisis in Legal Representation of Birth Parents in Child Protective ProceedingsRick ThomaОценок пока нет
- Elisa W V NYC Foster Care Suit Consent Decree 10-20-15Документ18 страницElisa W V NYC Foster Care Suit Consent Decree 10-20-15Rick ThomaОценок пока нет
- Walker - Dept. of Justice Amicus Curae BriefДокумент34 страницыWalker - Dept. of Justice Amicus Curae BriefGrant SternОценок пока нет
- Commission of Investigation Mother and Baby Homes Order Jan 2015Документ10 страницCommission of Investigation Mother and Baby Homes Order Jan 2015Rick ThomaОценок пока нет
- AR V Interim Care Foster Family Agency Civil Complaint June 25 2015Документ70 страницAR V Interim Care Foster Family Agency Civil Complaint June 25 2015Rick ThomaОценок пока нет
- Elisa W V City of New York Class Action ComplaintДокумент256 страницElisa W V City of New York Class Action ComplaintRick ThomaОценок пока нет
- Polk County Grand Jury Report Highlands Youth Academy 2015Документ21 страницаPolk County Grand Jury Report Highlands Youth Academy 2015Rick ThomaОценок пока нет
- Marin County GJ Shining A Light On Foster Care 2014Документ14 страницMarin County GJ Shining A Light On Foster Care 2014Rick ThomaОценок пока нет
- Jones Et Al V Interim Care Foster Family Agency Oct 27 2014 PDFДокумент79 страницJones Et Al V Interim Care Foster Family Agency Oct 27 2014 PDFRick ThomaОценок пока нет
- Proposed Commission To Inquire Into Mother and Baby Homes Submission of The IHRCДокумент16 страницProposed Commission To Inquire Into Mother and Baby Homes Submission of The IHRCRick ThomaОценок пока нет
- Maryland DHR Pre Proposal Conference Child Support RevMax 2013Документ69 страницMaryland DHR Pre Proposal Conference Child Support RevMax 2013Rick ThomaОценок пока нет
- Report On Symphysiotomy in Ireland 1944-1984 (May 2013)Документ114 страницReport On Symphysiotomy in Ireland 1944-1984 (May 2013)Rick ThomaОценок пока нет
- Report of The Inter-Departmental Group On Mother and Baby Homes-June 2014Документ37 страницReport of The Inter-Departmental Group On Mother and Baby Homes-June 2014Rick ThomaОценок пока нет
- CA Senate Foster Care Psychotropic Hearing Background Paper 2015Документ13 страницCA Senate Foster Care Psychotropic Hearing Background Paper 2015Rick ThomaОценок пока нет
- 1991-92 San Diego County Grand Jury - Report 7, The Crisis in Foster CareДокумент21 страница1991-92 San Diego County Grand Jury - Report 7, The Crisis in Foster CareRick ThomaОценок пока нет
- Ex Parte Amber Lovill Tex App 13th Dist Opinion Dec 22 2008Документ26 страницEx Parte Amber Lovill Tex App 13th Dist Opinion Dec 22 2008Rick Thoma100% (1)
- Maryland DHR Pre Proposal Conference SSI Foster Care RevMax Oct 2014Документ74 страницыMaryland DHR Pre Proposal Conference SSI Foster Care RevMax Oct 2014Rick ThomaОценок пока нет
- HHS DOJ Mass DCF Letter Sara Gordon Ada Inevtigation Jan 2015Документ26 страницHHS DOJ Mass DCF Letter Sara Gordon Ada Inevtigation Jan 2015Rick Thoma100% (1)
- San Diego Grand Jury, Transitional Age Youth, 2010Документ8 страницSan Diego Grand Jury, Transitional Age Youth, 2010Rick ThomaОценок пока нет
- Ex Parte Amber Lovill Tex App 13th Dist Opinion Dec 22 2008Документ26 страницEx Parte Amber Lovill Tex App 13th Dist Opinion Dec 22 2008Rick Thoma100% (1)
- Tulare County Grand Jury Final Report 2013 2014Документ174 страницыTulare County Grand Jury Final Report 2013 2014Rick ThomaОценок пока нет
- San Joaquin County Grand Jury 2013 2014Документ226 страницSan Joaquin County Grand Jury 2013 2014Rick ThomaОценок пока нет
- Contra Costa Grand Jury, Our Foster Care Children in Jeopardy, 2010Документ4 страницыContra Costa Grand Jury, Our Foster Care Children in Jeopardy, 2010Rick ThomaОценок пока нет
- FN2409 2706 - Footnotes Levin-Coburn Report.Документ975 страницFN2409 2706 - Footnotes Levin-Coburn Report.Rick ThomaОценок пока нет
- Sacramento Grand Jury, CPS: Nothing Ever Changes... Ever, 2009Документ31 страницаSacramento Grand Jury, CPS: Nothing Ever Changes... Ever, 2009Rick ThomaОценок пока нет
- FN107-1342 - Footnotes Levin-Coburn Report.Документ1 037 страницFN107-1342 - Footnotes Levin-Coburn Report.Rick ThomaОценок пока нет
- Barangay Ordinance On Videoke 2014Документ4 страницыBarangay Ordinance On Videoke 2014Renz Carlo0% (1)
- 4 TH CreterionДокумент29 страниц4 TH CreterionAlumni GECОценок пока нет
- California State Fire Marshal CODE INTERPRETATIONДокумент2 страницыCalifornia State Fire Marshal CODE INTERPRETATIONJohn simpsonОценок пока нет
- PUP College Entrance TestДокумент5 страницPUP College Entrance TestJoanamarie Kabiling88% (8)
- Gurpreet ResumeДокумент3 страницыGurpreet ResumeKavi rajputОценок пока нет
- Action Plan For S2-SFIST JOel L Navarro1Документ4 страницыAction Plan For S2-SFIST JOel L Navarro1Rico EsponillaОценок пока нет
- ANC UmrabuloДокумент224 страницыANC UmrabuloCityPressОценок пока нет
- Jamieson, Managing Director at Nielsen PhilippinesДокумент5 страницJamieson, Managing Director at Nielsen PhilippinesJohn Mark ZambranoОценок пока нет
- Computers & Industrial Engineering: Ming K. Lim, Yan Li, Chao Wang, Ming-Lang TsengДокумент14 страницComputers & Industrial Engineering: Ming K. Lim, Yan Li, Chao Wang, Ming-Lang TsengA. SajadiОценок пока нет
- Purchasing and ProcurementДокумент2 страницыPurchasing and ProcurementMarie Jeannie Intal100% (1)
- 3 6 3 1 Disaster Operations CenterДокумент7 страниц3 6 3 1 Disaster Operations CenterLorenzo Raphael C. ErlanoОценок пока нет
- Written Results of National Defence Academy and Naval Academy Examination (I), 2019Документ18 страницWritten Results of National Defence Academy and Naval Academy Examination (I), 2019Zee News100% (1)
- Lecture Note-Research Methods and Scientific Writing-2021Документ234 страницыLecture Note-Research Methods and Scientific Writing-2021addisu andargieОценок пока нет
- Transit Capacity and Quality of Service Manual, Third EditionДокумент2 страницыTransit Capacity and Quality of Service Manual, Third EditionkhanОценок пока нет
- Adoc - Pub - Information Sheet Name of The University J Selye UДокумент27 страницAdoc - Pub - Information Sheet Name of The University J Selye Ubernard aryaОценок пока нет
- Teachers and Their Security of TenureДокумент2 страницыTeachers and Their Security of TenureJoanna Marie Alfaras100% (3)
- Industrial Marketing Unit 1Документ10 страницIndustrial Marketing Unit 1scribdranijОценок пока нет
- Logistics Infrastructure of HaryanaДокумент20 страницLogistics Infrastructure of HaryanaEsha GuptaОценок пока нет
- Complaint Letter &asking For Price QuotationДокумент3 страницыComplaint Letter &asking For Price QuotationS.M. YAMINUR RAHMANОценок пока нет
- TestДокумент232 страницыTestseanmark87Оценок пока нет
- DOM CDCR Operations ManualДокумент188 страницDOM CDCR Operations ManualElisha Mc BrideОценок пока нет
- Other Disclosures and AuthorizationsДокумент13 страницOther Disclosures and AuthorizationsANKIT SINGHОценок пока нет
- TLE G7&8 Household Services PDFДокумент34 страницыTLE G7&8 Household Services PDFBhabz Malabz100% (8)
- In The International Criminal Court The Hague, The NetherlandsДокумент36 страницIn The International Criminal Court The Hague, The NetherlandssuhanaОценок пока нет
- Statement of Purpose Ib NikhilДокумент2 страницыStatement of Purpose Ib NikhilNikhil Kumar50% (2)
- Saep 120Документ4 страницыSaep 120Demac Saud0% (1)
- Chapter 4 PMP StudyДокумент24 страницыChapter 4 PMP StudyAbdülhamit KayyaliОценок пока нет
- CISM Certification Study Guide Part 1Документ24 страницыCISM Certification Study Guide Part 1AAA75% (4)
- Harry Chambers, Harry E. Chambers - Effective Communication Skills For Scientific and Technical Professionals-Basic Books (2000)Документ334 страницыHarry Chambers, Harry E. Chambers - Effective Communication Skills For Scientific and Technical Professionals-Basic Books (2000)Debaleena Dutta100% (4)
- Order Granting DismissalДокумент19 страницOrder Granting DismissalJim SchutzeОценок пока нет