Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Classifications of Heart MurmursДокумент2 страницыClassifications of Heart MurmursVS100% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Davidson's McqsДокумент145 страницDavidson's McqsSekhons Akademy100% (3)
- Step by Step Echocardiography in Congenital Heart DiseasesДокумент224 страницыStep by Step Echocardiography in Congenital Heart DiseasesEbookStore.DocОценок пока нет
- Radiology MCQSДокумент23 страницыRadiology MCQSHabib Mughal67% (3)
- Robbins Chapter 11Документ5 страницRobbins Chapter 11Luming LiОценок пока нет
- Urine Analysis FinalДокумент112 страницUrine Analysis FinalNischita JayarajОценок пока нет
- Assessment Nursing Diagnosis Planning Interventions Rationale EvaluationsДокумент3 страницыAssessment Nursing Diagnosis Planning Interventions Rationale EvaluationsAjay SupanОценок пока нет
- B.SC Degree Course in Nursing (Basic) Medical - Surgical Nursing - II Unit - X Occupational Lung DiseasesДокумент101 страницаB.SC Degree Course in Nursing (Basic) Medical - Surgical Nursing - II Unit - X Occupational Lung DiseasesvigneshОценок пока нет
- YeastДокумент2 страницыYeastAdriene Fay DominguezОценок пока нет
- A Study of An Existing Online Reservation of Tolentino's CateringДокумент12 страницA Study of An Existing Online Reservation of Tolentino's CateringAdriene Fay DominguezОценок пока нет
- Prof AdДокумент10 страницProf AdAdriene Fay DominguezОценок пока нет
- Bag TechniqueДокумент5 страницBag TechniqueAdriene Fay DominguezОценок пока нет
- Acute PainДокумент5 страницAcute PainAdriene Fay DominguezОценок пока нет
- FINAL Drug StudyДокумент8 страницFINAL Drug StudyAdriene Fay DominguezОценок пока нет
- Nutrition HTPДокумент3 страницыNutrition HTPAdriene Fay DominguezОценок пока нет
- National Institute On AgingДокумент8 страницNational Institute On AgingAdriene Fay DominguezОценок пока нет
- What Is ECG?Документ2 страницыWhat Is ECG?Lê Thanh HàОценок пока нет
- Child Proposal Form PDFДокумент9 страницChild Proposal Form PDFRaja SekarОценок пока нет
- Medical Surgical Nursing An Integrated Approach 3rd Edition White Test BankДокумент12 страницMedical Surgical Nursing An Integrated Approach 3rd Edition White Test Bankpauldiamondwe8100% (29)
- Mendelson's SyndromeДокумент17 страницMendelson's SyndromeMeena ViswaОценок пока нет
- Autoregulation of The Cardiovascular SystemДокумент15 страницAutoregulation of The Cardiovascular SystemErinne DefrianiОценок пока нет
- Mertoglu and Gunay 2017Документ5 страницMertoglu and Gunay 2017Via MeysaОценок пока нет
- Thorax - BRS Gross Anatomy NOTESДокумент8 страницThorax - BRS Gross Anatomy NOTESJustyna PoznanskaОценок пока нет
- Respiratory SystemДокумент61 страницаRespiratory SystemDenise Nicole PinedaОценок пока нет
- Fenofibratesimvastatin Fixed-Dose Combination in TДокумент13 страницFenofibratesimvastatin Fixed-Dose Combination in TMade DeanaОценок пока нет
- Obstetrics - MCQ - 3rd - BHMS - (Old, New, 2015)Документ25 страницObstetrics - MCQ - 3rd - BHMS - (Old, New, 2015)Anil kadamОценок пока нет
- Infective EndocarditisДокумент3 страницыInfective EndocarditisRechelle CabagingОценок пока нет
- Heart EksДокумент11 страницHeart EksAndri FerdianОценок пока нет
- BSN 3 C AssignmentДокумент2 страницыBSN 3 C AssignmentLeslie PaguioОценок пока нет
- Dialysis Hypotension Is The Result of AnДокумент4 страницыDialysis Hypotension Is The Result of AnCathy ManicadОценок пока нет
- 2021 WACP RecallДокумент48 страниц2021 WACP RecallAbdu-Raheem Fadlulai100% (1)
- Al-Shifa Hospital Cardiac Cath. Department: Labetalol Hydrochloride 5mg/ml Solution For InjectionДокумент2 страницыAl-Shifa Hospital Cardiac Cath. Department: Labetalol Hydrochloride 5mg/ml Solution For InjectionIyas JehadОценок пока нет
- 24 de AgostoДокумент7 страниц24 de Agostoapi-626131140Оценок пока нет
- RIVAL Study DesignДокумент11 страницRIVAL Study DesignggfraijОценок пока нет
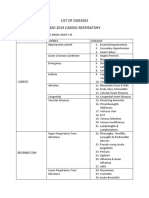
- List of Diseases Imo 2019 Cardio-RespiratoryДокумент2 страницыList of Diseases Imo 2019 Cardio-RespiratoryDimas Adjie Yuda MahendraОценок пока нет
- Shazia Kazi ResumeДокумент2 страницыShazia Kazi Resumeshazia kaziОценок пока нет
- Semaglutide For The Treatment of ObesityДокумент8 страницSemaglutide For The Treatment of ObesityNewtonRibeiroОценок пока нет
- Mesenteric Ischemia 1Документ11 страницMesenteric Ischemia 1Manuel E. Niebles De AyoОценок пока нет