Вам также может понравиться
- NBC September 2023 Poll For Release 92423Документ24 страницыNBC September 2023 Poll For Release 92423Veronica SilveriОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Quality Assurance in BacteriologyДокумент28 страницQuality Assurance in BacteriologyAuguz Francis Acena50% (2)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Lexis. Word Formation Features in English. Prefixation, Suffixation, and Compounding.Документ76 страницLexis. Word Formation Features in English. Prefixation, Suffixation, and Compounding.María Regal Carballo100% (3)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
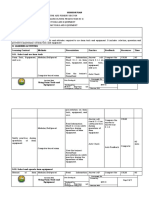
- PE Assessment Plan 1-2Документ1 страницаPE Assessment Plan 1-2Rhuvy RamosОценок пока нет
- Popular English Grammar Books: Want To ReadДокумент2 страницыPopular English Grammar Books: Want To ReadkatnavОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Weber's "Protestant Ethic" and His Critics by Ethan CrowellДокумент63 страницыWeber's "Protestant Ethic" and His Critics by Ethan Crowellcalatorul70100% (1)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Law School Academic Calendar S Y 2017-2018 First Semester: June 5, 2017 - October 6, 2017Документ25 страницLaw School Academic Calendar S Y 2017-2018 First Semester: June 5, 2017 - October 6, 2017nvmndОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Aiming For Integrity Answer GuideДокумент4 страницыAiming For Integrity Answer GuidenagasmsОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Hit ParadeДокумент20 страницHit ParadeNishant JainОценок пока нет
- 10 Global Trends in ICT and EducationДокумент3 страницы10 Global Trends in ICT and Educationmel m. ortiz0% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- User Centered Design Assessment by JokelaДокумент13 страницUser Centered Design Assessment by JokelaIdyawati HusseinОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Skillful LS4 Unit 4 Test - EditableДокумент4 страницыSkillful LS4 Unit 4 Test - EditableHoa NguyễnОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Ba7101 - PomДокумент7 страницBa7101 - PomanglrОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- DLP DIASS Q2 Week B-D - Functions of Applied Social Sciences 3Документ7 страницDLP DIASS Q2 Week B-D - Functions of Applied Social Sciences 3Paolo Bela-ongОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Child Development in UAEДокумент6 страницChild Development in UAEkelvin fabichichiОценок пока нет
- Contoh Pidato Bahasa InggrisДокумент2 страницыContoh Pidato Bahasa Inggrisalice_dmcОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Peace Corps Dominican Republic Welcome Book - December 2011CCD Updated June 13, 2013 DOWB517Документ50 страницPeace Corps Dominican Republic Welcome Book - December 2011CCD Updated June 13, 2013 DOWB517Accessible Journal Media: Peace Corps DocumentsОценок пока нет
- Group Dynamics and Teamwork: Ian GrigorДокумент15 страницGroup Dynamics and Teamwork: Ian GrigorKhabir IslamОценок пока нет
- Climate Change Webquest RubricДокумент1 страницаClimate Change Webquest Rubricapi-3554784500% (1)
- Best Practices (Sraes)Документ19 страницBest Practices (Sraes)encarОценок пока нет
- A UCSP Q1M6 Teacher Copy Final LayoutДокумент25 страницA UCSP Q1M6 Teacher Copy Final LayoutKarylle Joy DumalaganОценок пока нет
- Cengage LearningДокумент12 страницCengage LearningerikomarОценок пока нет
- Teaching LoadsДокумент20 страницTeaching LoadsZean ZeusОценок пока нет
- Bab II ProposalДокумент4 страницыBab II ProposalMawaddah HidayatiОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- CHED Puroposive CommunicationДокумент13 страницCHED Puroposive CommunicationCyril-J BalboaОценок пока нет
- Obembe Adebola's Personal StatementДокумент1 страницаObembe Adebola's Personal Statementeunice bimpeОценок пока нет
- A Proposed Program To Prevent Violence Against Women (Vaw) in Selected Barangays of Batangas CityДокумент16 страницA Proposed Program To Prevent Violence Against Women (Vaw) in Selected Barangays of Batangas CityMarimarjnhioОценок пока нет
- My HanumanДокумент70 страницMy Hanumanrajeshlodi100% (1)
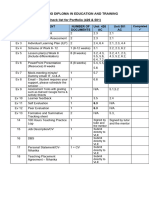
- Checklist For Portfolio Evidence (426 & 501) (Final)Документ1 страницаChecklist For Portfolio Evidence (426 & 501) (Final)undan.uk3234Оценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Lo2. Using Farm Tools and EquipmentДокумент8 страницLo2. Using Farm Tools and Equipmentrobelyn veranoОценок пока нет