Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- VitaminsДокумент13 страницVitaminsمحمد ابوالمجدОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Biologic Width - The No Encroachment Zone: I J D AДокумент8 страницBiologic Width - The No Encroachment Zone: I J D AJinny ShawОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- 4 3 937Документ4 страницы4 3 937محمد ابوالمجدОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Guidelines On Infection Control in Dental ClinicsДокумент10 страницGuidelines On Infection Control in Dental ClinicsHare RamОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- ChemFil Superior44Документ27 страницChemFil Superior44محمد ابوالمجدОценок пока нет
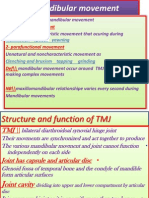
- Mandibular MovementДокумент4 страницыMandibular Movementمحمد ابوالمجدОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- VitaminsДокумент13 страницVitaminsمحمد ابوالمجدОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Smear LayerДокумент9 страницSmear Layerpriyanka_gedamОценок пока нет
- Behaviour Management 2Документ59 страницBehaviour Management 2Nikhil RaiОценок пока нет
- Dental Anatomy DecksДокумент362 страницыDental Anatomy Decksapi-2629165183% (6)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Dental Cements For UseДокумент28 страницDental Cements For UseAhmed DolaОценок пока нет
- Anatomy of CNSДокумент32 страницыAnatomy of CNSLeonita AguillonОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Anatomy of CNSДокумент32 страницыAnatomy of CNSLeonita AguillonОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Publication PDFДокумент28 страницPublication PDFمحمد ابوالمجدОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Publication PDFДокумент20 страницPublication PDFمحمد ابوالمجدОценок пока нет
- 1Документ15 страниц1محمد ابوالمجدОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Finishing and PolishingДокумент18 страницFinishing and Polishingab0maiОценок пока нет
- Dental Management of Medically Compromised PatientsДокумент12 страницDental Management of Medically Compromised Patientsمحمد ابوالمجدОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Mandibular MovementДокумент4 страницыMandibular Movementمحمد ابوالمجدОценок пока нет
- DentistryДокумент71 страницаDentistryAnupama NagrajОценок пока нет
- Anatomy of CNSДокумент32 страницыAnatomy of CNSLeonita AguillonОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Emergency MedicineДокумент7 страницEmergency Medicineمحمد ابوالمجدОценок пока нет
- Asnan 7 RulesДокумент2 страницыAsnan 7 Rulesمحمد ابوالمجدОценок пока нет
- OcclusionДокумент17 страницOcclusionمحمد ابوالمجدОценок пока нет
- MCQPaperSept 05Документ4 страницыMCQPaperSept 05api-26291651100% (1)
- Serial Extraction PedoДокумент23 страницыSerial Extraction PedoSelim BaftiuОценок пока нет
- Tooth MovementДокумент14 страницTooth Movementمحمد ابوالمجدОценок пока нет
- MCQSeptember 2006 Paper IДокумент3 страницыMCQSeptember 2006 Paper Iapi-26291651100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Etiology of MalocclusionДокумент28 страницEtiology of MalocclusionPriyaancaHaarsh100% (3)
- RO0111 00-00 WebberДокумент6 страницRO0111 00-00 WebberARTОценок пока нет
- SIALOGRAPHY EXAMINATION Kel 3Документ17 страницSIALOGRAPHY EXAMINATION Kel 3Ratih susilowatiОценок пока нет
- Cluster 3 - Sre RRT2022Документ135 страницCluster 3 - Sre RRT2022Rosie RojasОценок пока нет
- Sialolithiasis: Radiological Diagnosis and Treatment: NovemberДокумент33 страницыSialolithiasis: Radiological Diagnosis and Treatment: NovemberAciih HeHoОценок пока нет
- SALIVARY GLAND IMAGING-Seminar ConversionДокумент114 страницSALIVARY GLAND IMAGING-Seminar ConversionVanshika JainОценок пока нет
- Radiographic Special ProceduresДокумент211 страницRadiographic Special ProceduresPrincess Joy CamposОценок пока нет
- The Erlangen Salivary Gland Project: Part I: Sialendoscopy in Obstructive Diseases of The Major Salivary GlandsДокумент60 страницThe Erlangen Salivary Gland Project: Part I: Sialendoscopy in Obstructive Diseases of The Major Salivary GlandsRosa Silva100% (1)
- Maxillary Sinus Disease - Power Point PresentationДокумент45 страницMaxillary Sinus Disease - Power Point PresentationRohan Grover100% (1)
- Sialography Conventional, CT, MriДокумент54 страницыSialography Conventional, CT, Mrishivubir100% (1)
- K. Graamans, H. P. Van Den Akker (Auth.), K. Graamans, H. P. Van Den Akker (Eds.) - Diagnosis of Salivary Gland Disorders-Springer Netherlands (1991)Документ182 страницыK. Graamans, H. P. Van Den Akker (Auth.), K. Graamans, H. P. Van Den Akker (Eds.) - Diagnosis of Salivary Gland Disorders-Springer Netherlands (1991)Sangam AdhikariОценок пока нет
- Master Radiology Notes GIT PDFДокумент115 страницMaster Radiology Notes GIT PDFuroshkgОценок пока нет
- Diagnose of Submandibular Abscess PDFДокумент13 страницDiagnose of Submandibular Abscess PDFElvitrianaОценок пока нет
- Sialography ExaminationДокумент14 страницSialography ExaminationEkaRahmaОценок пока нет
- Sublingual Sialocele in A Cat: Jean Bassanino, Sophie Palierne, Margaux Blondel and Brice S ReynoldsДокумент5 страницSublingual Sialocele in A Cat: Jean Bassanino, Sophie Palierne, Margaux Blondel and Brice S ReynoldsTarsilaRibeiroMaiaОценок пока нет
- Contrast Agents in DentistryДокумент45 страницContrast Agents in DentistryPushkar DahiwalОценок пока нет