Вам также может понравиться
- Abdominal Pain Content PDFДокумент71 страницаAbdominal Pain Content PDFyanОценок пока нет
- Cancer Basics PDFДокумент16 страницCancer Basics PDFPrashant Chari100% (1)
- Cancer BiomarkersДокумент7 страницCancer Biomarkersmaheen_aslam6596Оценок пока нет
- Boala Paget A Glandei MamareДокумент41 страницаBoala Paget A Glandei MamarePANNADYОценок пока нет
- Breast Cancer Staging PDFДокумент12 страницBreast Cancer Staging PDFDanu BagoesОценок пока нет
- Cervical Cancer in PregnancyДокумент21 страницаCervical Cancer in Pregnancymineresearch100% (1)
- D105 APBI Future - My Point of ViewДокумент70 страницD105 APBI Future - My Point of ViewSoc. Portuguesa de Radioterapia OncologiaОценок пока нет
- Management of High Grade Bladder Cancer & Carcinoma in SituДокумент26 страницManagement of High Grade Bladder Cancer & Carcinoma in SituSakuntalaPalankiОценок пока нет
- Introduction of Clinical OncologyДокумент52 страницыIntroduction of Clinical OncologyThis is Pony100% (1)
- Folfiri Beva Gi Col PДокумент12 страницFolfiri Beva Gi Col Pvera docОценок пока нет
- Principle of Chemotherapy Main PresentationДокумент84 страницыPrinciple of Chemotherapy Main Presentationadekunle ajayiОценок пока нет
- Carboplatin PaclitaxelДокумент6 страницCarboplatin PaclitaxelNida Auliya RahmahОценок пока нет
- Clinical Presentation, Diagnosis, and Staging of Colorectal Cancer - UpToDate PDFДокумент41 страницаClinical Presentation, Diagnosis, and Staging of Colorectal Cancer - UpToDate PDFVali MocanuОценок пока нет
- Japanese Classification of Esophageal CancerДокумент25 страницJapanese Classification of Esophageal CancerppcloverОценок пока нет
- Thromboembolism & ThromboprophylaxisДокумент48 страницThromboembolism & Thromboprophylaxisazida90Оценок пока нет
- Breast Cancer: Prima Medika HospitalДокумент35 страницBreast Cancer: Prima Medika HospitalPrima MedikaОценок пока нет
- Breast Cancer in Women - A Narrative Literature ReviewДокумент7 страницBreast Cancer in Women - A Narrative Literature ReviewAnnie McSolsticeОценок пока нет
- Management of Breast CancerДокумент53 страницыManagement of Breast CancerGaoudam NatarajanОценок пока нет
- BC CancerДокумент42 страницыBC CancerIsal SparrowОценок пока нет
- Molecular Diagnostics in Cancer Paper 1Документ15 страницMolecular Diagnostics in Cancer Paper 1Marian ValdiviaОценок пока нет
- Cancer PainДокумент14 страницCancer PainPratita Jati PermatasariОценок пока нет
- Anal CancerДокумент14 страницAnal Cancerdrsp2001Оценок пока нет
- Oncology-Study of Cancer Cellular AbberationДокумент43 страницыOncology-Study of Cancer Cellular AbberationIrwan M. IskoberОценок пока нет
- Cancer: Causes and Risks FactorsДокумент88 страницCancer: Causes and Risks FactorsClancy Anne Garcia NavalОценок пока нет
- Overview of CancerДокумент31 страницаOverview of Cancersamarth kaulОценок пока нет
- Local Management of Invasive Breast Cancer: by Steven Jones, MDДокумент37 страницLocal Management of Invasive Breast Cancer: by Steven Jones, MDsrikadarinahОценок пока нет
- Adenoid Cystic CarcinomaДокумент7 страницAdenoid Cystic CarcinomalonadiolandaОценок пока нет
- Sentinel Lymph Node ConceptДокумент27 страницSentinel Lymph Node ConceptKarthikeyan RadhakrishnanОценок пока нет
- Medicine2 - Complications of Cancer Treatment 2007Документ76 страницMedicine2 - Complications of Cancer Treatment 2007api-3762917Оценок пока нет
- Breast Cancer DetectionДокумент5 страницBreast Cancer DetectionalexlingmanchesterОценок пока нет
- (R) Choep: IndicationДокумент5 страниц(R) Choep: IndicationAlina CrissОценок пока нет
- Skin Cancer in HKДокумент6 страницSkin Cancer in HKChiu ChunОценок пока нет
- Diagnosis and Treatment of MelanomaДокумент14 страницDiagnosis and Treatment of MelanomaAnonymous Af24L7Оценок пока нет
- Concurrent ChemoRadiotherapyДокумент51 страницаConcurrent ChemoRadiotherapyJalal EltabibОценок пока нет
- Cancer Prevention, Screening, & Early DetectionДокумент13 страницCancer Prevention, Screening, & Early Detectionchfalguera100% (1)
- Locally Advanced Breast CarcinomaДокумент31 страницаLocally Advanced Breast Carcinomaapi-3701915100% (1)
- Spontaneous Regression of Pancreatic Cancer: A Case Report and Literature ReviewДокумент5 страницSpontaneous Regression of Pancreatic Cancer: A Case Report and Literature ReviewHitomi-Оценок пока нет
- Cell Cycle ChemotherapyДокумент5 страницCell Cycle ChemotherapyVictoria Alessandra BrownОценок пока нет
- ILRT Dr. Sarbani-1 PDFДокумент48 страницILRT Dr. Sarbani-1 PDFdurgesh kumar100% (1)
- Cervical Intraepithelial Neoplasia and Cervical CancerДокумент28 страницCervical Intraepithelial Neoplasia and Cervical CancerNatnael100% (1)
- 4 Lung-CancerДокумент72 страницы4 Lung-CancerTaima FayezОценок пока нет
- Breast CancerДокумент27 страницBreast CancerSusmita PalОценок пока нет
- Breast Cancer: Screening and PreventionДокумент32 страницыBreast Cancer: Screening and Preventionwalter agyemanОценок пока нет
- If HP Cancer Guide br007 MriДокумент13 страницIf HP Cancer Guide br007 Mrirusgal8992100% (1)
- Awareness of Breast Cancer Symptoms Among Women in The Southern African Development Community - FinalДокумент18 страницAwareness of Breast Cancer Symptoms Among Women in The Southern African Development Community - FinalMzati MphepoОценок пока нет
- Introductory Pharmacology - Cancer ChemotherapyДокумент9 страницIntroductory Pharmacology - Cancer ChemotherapyTyler Rosolowski100% (2)
- (Onco) Oncologic EmergenciesДокумент71 страница(Onco) Oncologic EmergencieshatsuneОценок пока нет
- Benign and Malignant Lesion of Lower GIДокумент45 страницBenign and Malignant Lesion of Lower GIAhmad Alzu3beОценок пока нет
- Breast Cancer Guidelines OverviewДокумент23 страницыBreast Cancer Guidelines OverviewRodney MatthewsОценок пока нет
- Chemotherapy Protocols and Infusion Sequence Schedule Considerations in Cancer TreatmentДокумент330 страницChemotherapy Protocols and Infusion Sequence Schedule Considerations in Cancer TreatmentVirgilio Rafael Tovar Vasquez100% (4)
- Management of Breast CAДокумент22 страницыManagement of Breast CAAlma FarhanaОценок пока нет
- Anxiety and Depression After Cancer DiagnosisДокумент26 страницAnxiety and Depression After Cancer DiagnosisMesias PatricioОценок пока нет
- Colon PolypsДокумент28 страницColon PolypsDipОценок пока нет
- Xodo Document - Periprocedural - Anticoagulation - GuidelineДокумент16 страницXodo Document - Periprocedural - Anticoagulation - Guidelinebrigde_xОценок пока нет
- Case Study Breast CancerДокумент3 страницыCase Study Breast CancerJustin Joshua Derilo OrdoñaОценок пока нет
- Cervical CancerДокумент36 страницCervical CancerDebabrata SatapathyОценок пока нет
- Trimodality Therapy in Bladder CancerДокумент12 страницTrimodality Therapy in Bladder CancerStirОценок пока нет
- Breast Cancer Histologic SubtypesДокумент24 страницыBreast Cancer Histologic Subtypesgaby andreaОценок пока нет
- The American Cancer Society's Principles of Oncology: Prevention to SurvivorshipОт EverandThe American Cancer Society's Principles of Oncology: Prevention to SurvivorshipThe American Cancer SocietyОценок пока нет
- Hyperglycemia in PregnancyДокумент17 страницHyperglycemia in PregnancyIza WidzОценок пока нет
- GE Voluson e PDFДокумент9 страницGE Voluson e PDFJames López TorresОценок пока нет
- Postpartal Pueperal InfectionДокумент38 страницPostpartal Pueperal InfectionIrish Jane Bayle CubilloОценок пока нет
- RPTДокумент6 страницRPTparagkulkarni11Оценок пока нет
- POSTTERM PREGNANCY or Prolonged Pregnancy I. Definition: Postmaturity SyndromeДокумент13 страницPOSTTERM PREGNANCY or Prolonged Pregnancy I. Definition: Postmaturity SyndromeArjay AmbaОценок пока нет
- WHO:SURGICAL WORKFORCE IN INDIA-What The State of Kerala Tells Us About The Production, Stock and Migration of The Health WorkforceДокумент33 страницыWHO:SURGICAL WORKFORCE IN INDIA-What The State of Kerala Tells Us About The Production, Stock and Migration of The Health Workforcemahwish khanОценок пока нет
- EPDSScoringGuide March2015 PDFДокумент1 страницаEPDSScoringGuide March2015 PDFantivenomОценок пока нет
- Complications Failures and Maintainence of Dental Implant 160218154535Документ45 страницComplications Failures and Maintainence of Dental Implant 160218154535DrIbrahimShaikhОценок пока нет
- MyomaДокумент40 страницMyomagaasheОценок пока нет
- Jindal HospitalДокумент61 страницаJindal HospitalGajula AnilОценок пока нет
- 85140-160 Erbe en Vio S D024761Документ8 страниц85140-160 Erbe en Vio S D024761Bogdan StraciucОценок пока нет
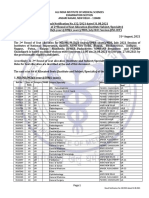
- 2nd Round Seat Allotment Result MDMS MDS Final NET2Документ52 страницы2nd Round Seat Allotment Result MDMS MDS Final NET2SARKAR JAVED AKHTARОценок пока нет
- Modified by Garnavos Milch Vs Kocher Technique For Anterior Shoulder DislocationДокумент9 страницModified by Garnavos Milch Vs Kocher Technique For Anterior Shoulder DislocationNick LasanianosОценок пока нет
- ICN Daily Round ChecklistДокумент1 страницаICN Daily Round ChecklistrenuОценок пока нет
- Gowri S Reasearch ProposalДокумент12 страницGowri S Reasearch ProposalzzzzОценок пока нет
- Le Garrot de Prelevement Chez Le Nouveau-Ne, Pas Toujours Anodin: A Propos de Deux CasДокумент6 страницLe Garrot de Prelevement Chez Le Nouveau-Ne, Pas Toujours Anodin: A Propos de Deux CasIJAR JOURNALОценок пока нет
- English: For The Students of Nursing ScienceДокумент63 страницыEnglish: For The Students of Nursing ScienceNguyễn Chí TâmОценок пока нет
- Periprosthetic Fractures of The Proximal Femur Beyond The Vancouver ClassificationДокумент8 страницPeriprosthetic Fractures of The Proximal Femur Beyond The Vancouver ClassificationDavidBeatonComuladaОценок пока нет
- Abnormal LaborДокумент20 страницAbnormal Laborأ.م.د. إنعام فيصل محمدОценок пока нет
- DONA International (1992-) : SourcesДокумент2 страницыDONA International (1992-) : SourcesInglês The Right WayОценок пока нет
- Bone RegenerationДокумент360 страницBone RegenerationMarc Balsells100% (1)
- CBCNДокумент87 страницCBCNRabi DhakalОценок пока нет
- The Essential Identity of The Klippel-Feil Syndrome and IniencephalyДокумент16 страницThe Essential Identity of The Klippel-Feil Syndrome and IniencephalyIsolda Alanna RlОценок пока нет
- Diabetes Mellitus - ICD-10 CodingДокумент14 страницDiabetes Mellitus - ICD-10 CodingTim T VargheseОценок пока нет
- Daftar PustakaДокумент2 страницыDaftar PustakaYuli ErmaОценок пока нет
- Fam CaseДокумент9 страницFam Casefam111222Оценок пока нет
- Endotracheal TubeДокумент23 страницыEndotracheal Tubeanayunita100% (1)
- High Risk Neonatal Nursing CareДокумент40 страницHigh Risk Neonatal Nursing Carecarol_cezar100% (2)
- The Preoperative EvaluationДокумент25 страницThe Preoperative Evaluationnormie littlemonsterОценок пока нет