Вам также может понравиться
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Peter Wolf - History of Epilepsy - Nosological Concepts and ClassificationДокумент9 страницPeter Wolf - History of Epilepsy - Nosological Concepts and Classificationgoo99Оценок пока нет
- Visual IndeterminacyДокумент16 страницVisual Indeterminacygoo99Оценок пока нет
- Cobra Sheet - ZornДокумент2 страницыCobra Sheet - Zorngoo99Оценок пока нет
- Le VanQuyen - Neurodynamics and Phenomenology in Mutual Enlightenment: The Example of The Epileptic Aura.Документ25 страницLe VanQuyen - Neurodynamics and Phenomenology in Mutual Enlightenment: The Example of The Epileptic Aura.goo99Оценок пока нет
- Sound of Cinema, SOUND OF CINEMA: THE MUSIC THAT MADE THE MOVIESДокумент9 страницSound of Cinema, SOUND OF CINEMA: THE MUSIC THAT MADE THE MOVIESgoo99Оценок пока нет
- Ictal and Postictal Psychiatric Disturbances - TrimbleДокумент5 страницIctal and Postictal Psychiatric Disturbances - Trimblegoo99Оценок пока нет
- Synchronousobjects For One Flat Thing, Reproduced by William ForsytheДокумент4 страницыSynchronousobjects For One Flat Thing, Reproduced by William Forsythegoo99Оценок пока нет
- GUIDE Equality and Human Rights CommissionДокумент60 страницGUIDE Equality and Human Rights CommissionAmanda MotaОценок пока нет
- Font Management in OS X by Kurt Lang, October 15, 2012, PDFДокумент34 страницыFont Management in OS X by Kurt Lang, October 15, 2012, PDFgoo99Оценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Baseball Stadium Financing SummaryДокумент1 страницаBaseball Stadium Financing SummarypotomacstreetОценок пока нет
- Surviving Hetzers G13Документ42 страницыSurviving Hetzers G13Mercedes Gomez Martinez100% (2)
- Marking SchemeДокумент8 страницMarking Schememohamed sajithОценок пока нет
- Service Index PDF - PHP Content Id 2378053&content Tid 388906138&content Type TempДокумент2 страницыService Index PDF - PHP Content Id 2378053&content Tid 388906138&content Type Tempshiripalsingh0167Оценок пока нет
- CG Road EscortsДокумент3 страницыCG Road EscortsNeha SharmaОценок пока нет
- Digest Pre TrialДокумент2 страницыDigest Pre TrialJei Essa AlmiasОценок пока нет
- Horizon Trial: Witness Statement in Support of Recusal ApplicationДокумент12 страницHorizon Trial: Witness Statement in Support of Recusal ApplicationNick Wallis100% (1)
- BPV Installation Inspection Request Form With Payment AuthorizationДокумент2 страницыBPV Installation Inspection Request Form With Payment AuthorizationBoriche DivitisОценок пока нет
- Tugas Etik Koas BaruДокумент125 страницTugas Etik Koas Baruriska suandiwiОценок пока нет
- Assignment 1Документ3 страницыAssignment 1Bahle DlaminiОценок пока нет
- Vayutel Case StudyДокумент10 страницVayutel Case StudyRenault RoorkeeОценок пока нет
- ICargo Mobility QantasДокумент4 страницыICargo Mobility QantasViswateja KrottapalliОценок пока нет
- Slavfile: in This IssueДокумент34 страницыSlavfile: in This IssueNora FavorovОценок пока нет
- Natural Is at Ion As A British Citizen MGHOCДокумент17 страницNatural Is at Ion As A British Citizen MGHOCAsad Ali KhanОценок пока нет
- Linking Social Science Theories/Models To EducationДокумент2 страницыLinking Social Science Theories/Models To EducationAlexa GandioncoОценок пока нет
- No Man An IslandДокумент10 страницNo Man An IslandIsabel ChiuОценок пока нет
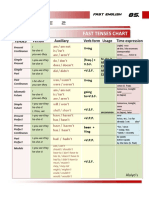
- Table 2: Fast Tenses ChartДокумент5 страницTable 2: Fast Tenses ChartAngel Julian HernandezОценок пока нет
- Ethical Dilemma Notes KiitДокумент4 страницыEthical Dilemma Notes KiitAritra MahatoОценок пока нет
- Spiritual Fitness Assessment: Your Name: - Date: - InstructionsДокумент2 страницыSpiritual Fitness Assessment: Your Name: - Date: - InstructionsLeann Kate MartinezОценок пока нет
- Why Study in USAДокумент4 страницыWhy Study in USALowlyLutfurОценок пока нет
- 1 s2.0 S0141391023000721 MainДокумент28 страниц1 s2.0 S0141391023000721 MainYemey Quispe ParedesОценок пока нет
- Busi Environment MCQДокумент15 страницBusi Environment MCQAnonymous WtjVcZCg57% (7)
- Full Download Health Psychology Theory Research and Practice 4th Edition Marks Test BankДокумент35 страницFull Download Health Psychology Theory Research and Practice 4th Edition Marks Test Bankquininemagdalen.np8y3100% (39)
- Solar - Bhanu Solar - Company ProfileДокумент9 страницSolar - Bhanu Solar - Company ProfileRaja Gopal Rao VishnudasОценок пока нет
- DIS Investment ReportДокумент1 страницаDIS Investment ReportHyperОценок пока нет
- Urban Transportation System Design and Feasibility Analysis A Case Study of Lagos Mega-CityДокумент8 страницUrban Transportation System Design and Feasibility Analysis A Case Study of Lagos Mega-CityKaren EstradaОценок пока нет
- Specific Relief Act, 1963Документ23 страницыSpecific Relief Act, 1963Saahiel Sharrma0% (1)
- ANA A. CHUA and MARCELINA HSIA, Complainants, vs. ATTY. SIMEON M. MESINA, JR., RespondentДокумент7 страницANA A. CHUA and MARCELINA HSIA, Complainants, vs. ATTY. SIMEON M. MESINA, JR., Respondentroyel arabejoОценок пока нет
- B. Contract of Sale: D. Fraud in FactumДокумент5 страницB. Contract of Sale: D. Fraud in Factumnavie VОценок пока нет
- 240 Marilag v. MartinezДокумент21 страница240 Marilag v. Martinezdos2reqjОценок пока нет