Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Nausea and Vomiting: Key ConceptsДокумент35 страницNausea and Vomiting: Key ConceptsMila ErnilaОценок пока нет
- CorticosteroidsДокумент63 страницыCorticosteroidsRiddhi Jain100% (2)
- Ozur DexДокумент3 страницыOzur DexMohammad Abdullah BawtagОценок пока нет
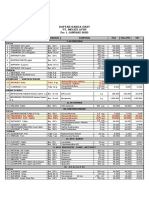
- Daftar Harga Obat - Pt. Molex Ayus - Januari 2023Документ4 страницыDaftar Harga Obat - Pt. Molex Ayus - Januari 2023Muhammad AdninОценок пока нет
- Lung Cancer Case StudyДокумент48 страницLung Cancer Case StudySahal M.Shuaib100% (4)
- Ivig GAMMARAS - FullДокумент13 страницIvig GAMMARAS - FullNisa UcilОценок пока нет
- Generic Name Brand Name Dosage Indications Mechanisms of Action Adverse Effects Nursing ResponsibilitiesДокумент10 страницGeneric Name Brand Name Dosage Indications Mechanisms of Action Adverse Effects Nursing ResponsibilitiesJennalyn CasapaoОценок пока нет
- Tobradex Eye Drops: Consumer Medicine InformationДокумент5 страницTobradex Eye Drops: Consumer Medicine InformationFranc VenturaОценок пока нет
- CorticoДокумент5 страницCorticoDR AbidОценок пока нет
- Idsa Covid 19 GL TX and MGMT v4.4.1Документ173 страницыIdsa Covid 19 GL TX and MGMT v4.4.1Galaxy SatwaОценок пока нет
- Perbandingan Dexa Dan MethylprednisoloneДокумент2 страницыPerbandingan Dexa Dan MethylprednisoloneRai Jaine DarmantaОценок пока нет
- Anatomy and Physiology Related To Multiple Myelom1Документ15 страницAnatomy and Physiology Related To Multiple Myelom1Diane Kate Tobias Magno100% (1)
- Pharmacokinetics: of OphthalmicДокумент4 страницыPharmacokinetics: of OphthalmicWina Siska Purnama BurmanОценок пока нет
- Steroid Side Effects - How To Reduce Corticosteroid Side Effects - HSSДокумент8 страницSteroid Side Effects - How To Reduce Corticosteroid Side Effects - HSSAtif RehmanОценок пока нет
- Mascc Antiemetic Guidelines English v.1.2.1Документ55 страницMascc Antiemetic Guidelines English v.1.2.1cricriОценок пока нет
- January 2021 Addendum To The Demonstration of The Falsified Romanian Drug and Human Trafficking Mafia Documents at ECHR September 2020Документ247 страницJanuary 2021 Addendum To The Demonstration of The Falsified Romanian Drug and Human Trafficking Mafia Documents at ECHR September 2020Tudor RanetiОценок пока нет
- PONV Prophylaxis GuidelinesДокумент7 страницPONV Prophylaxis GuidelinesAbby WardОценок пока нет
- Pharma 4 QДокумент1 страницаPharma 4 QMARIA PAULINA AMANTEОценок пока нет
- (Đề có 12 trang) : There are three parts in this listening test. You will hear each part twiceДокумент12 страниц(Đề có 12 trang) : There are three parts in this listening test. You will hear each part twiceTún PhạmОценок пока нет
- Multiple Myeloma ManuscriptДокумент36 страницMultiple Myeloma ManuscriptGabriel GuerreroОценок пока нет
- Guidline Mual Muntah Kemotrapi PDFДокумент10 страницGuidline Mual Muntah Kemotrapi PDFTyas TyaОценок пока нет
- Charlier Et Al. Lancet Infectious Diseases 2017Документ47 страницCharlier Et Al. Lancet Infectious Diseases 2017werwrОценок пока нет
- Drug LiteratureДокумент7 страницDrug LiteraturePatricia Anne BerganciaОценок пока нет
- Betnesol InjectionДокумент7 страницBetnesol Injectionhiral mistryОценок пока нет
- Drug StudyДокумент4 страницыDrug StudyJunel Paolo SilvioОценок пока нет
- Drugs Generally Used On Veterinary Clinics in IndiaДокумент17 страницDrugs Generally Used On Veterinary Clinics in IndiaDEV3LLS100% (1)
- Maxitrol (Neomycin and Polymyxin B Sulfates and Dexamethasone Ophthalmic Ointment) Sterile Description: MaxitrolДокумент6 страницMaxitrol (Neomycin and Polymyxin B Sulfates and Dexamethasone Ophthalmic Ointment) Sterile Description: Maxitroldjilal430Оценок пока нет
- Drug StudyДокумент7 страницDrug StudyNicxx GamingОценок пока нет
- End-of-Life Care For Brain Tumor PatientsДокумент36 страницEnd-of-Life Care For Brain Tumor PatientsNisha PradeepaОценок пока нет
- GP Factsheet - Steroids and The EyeДокумент6 страницGP Factsheet - Steroids and The EyeBima RizkiОценок пока нет