Вам также может понравиться
- Few Project TitlesДокумент7 страницFew Project TitlesRongalaSnehaОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Systematic Review of Diagnostic Utility and Therapeutic Effectiveness of Thoracic Facet Joint InterventionsДокумент19 страницSystematic Review of Diagnostic Utility and Therapeutic Effectiveness of Thoracic Facet Joint InterventionsRongalaSnehaОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Factsheet Common EquipmentДокумент2 страницыFactsheet Common EquipmentRongalaSnehaОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Chemical Safety Bio - Medical Waste Management Self Learning Document For Nurses and Paramedic AДокумент79 страницChemical Safety Bio - Medical Waste Management Self Learning Document For Nurses and Paramedic ARongalaSnehaОценок пока нет
- Self Assessment ToolkitДокумент39 страницSelf Assessment ToolkitRongalaSnehaОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Arogyasri HealthДокумент115 страницArogyasri Healthravind5Оценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- 1 Tools SpecificationsДокумент10 страниц1 Tools SpecificationsRongalaSnehaОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Group 5 Medical TourismДокумент27 страницGroup 5 Medical TourismRongalaSnehaОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Training Plan TemplateДокумент2 страницыTraining Plan Templateus_hazizi100% (3)
- Medical Records and The LawДокумент10 страницMedical Records and The LawRongalaSnehaОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Developing A Spa and Wellness BusinessДокумент21 страницаDeveloping A Spa and Wellness BusinessRongalaSnehaОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Biomedical Engineering: By: Justin Lau, Kaisen Nakagawa, Preston Iha and Nuuanu Tech ClubДокумент10 страницBiomedical Engineering: By: Justin Lau, Kaisen Nakagawa, Preston Iha and Nuuanu Tech ClubS.m. ChandrashekarОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Annex I National Leprosy Eradication ProgrammeДокумент5 страницAnnex I National Leprosy Eradication ProgrammespmdocОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Sobrecarga CuidadoresДокумент6 страницSobrecarga CuidadoresMARIA FRANCISCA VERGARA AGUILARОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
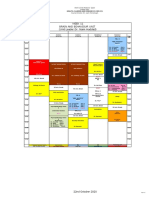
- Week 11 Brain and Behaviour Unit (Unit Leader:Dr. Naim Haddad)Документ1 страницаWeek 11 Brain and Behaviour Unit (Unit Leader:Dr. Naim Haddad)f3er3Оценок пока нет
- Advanced Health Care : Team-UtkorshoДокумент11 страницAdvanced Health Care : Team-UtkorshoIFTAKHARUL ISLAMОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Intern Annual16Документ7 страницIntern Annual16Akash PanwarОценок пока нет
- Clinical Research Organization / Contract Research OrganizationДокумент34 страницыClinical Research Organization / Contract Research OrganizationPHARMAIGNITEОценок пока нет
- Sanjay Gandhi Post Graduate Institute of Medical Sciences: Raebareli Road, Lucknow - 226 014, IndiaДокумент1 страницаSanjay Gandhi Post Graduate Institute of Medical Sciences: Raebareli Road, Lucknow - 226 014, IndiaAtul DubeyОценок пока нет
- IMD 2011 Class ProfileДокумент12 страницIMD 2011 Class ProfileDavid LewkowitzОценок пока нет
- Quality Assurance: Components of Quality Assurance - Tools in Quality AssuranceДокумент25 страницQuality Assurance: Components of Quality Assurance - Tools in Quality AssuranceBlaiseОценок пока нет
- Elderly CareДокумент63 страницыElderly Carehanfmhananfmhan100% (1)
- Medical Laboratory in Abu DhabiДокумент5 страницMedical Laboratory in Abu DhabiPrime CureОценок пока нет
- ReviewerДокумент3 страницыRevieweragustinadharleeОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Centric HealthДокумент38 страницCentric HealthJenny QuachОценок пока нет
- Management of Karnasrava - A Case ReportДокумент3 страницыManagement of Karnasrava - A Case ReportEditor IJTSRDОценок пока нет
- PCPNC BemoncДокумент180 страницPCPNC BemoncBeryl de la CruzОценок пока нет
- The Pittsburgh Sleep Quality Index PsqiДокумент2 страницыThe Pittsburgh Sleep Quality Index PsqiUswatun Hasanah IIОценок пока нет
- Diver Medical - Physician S Evaluation FormДокумент1 страницаDiver Medical - Physician S Evaluation Formcrispin quadrosОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Q2 Periodicaltest Mapeh10Документ5 страницQ2 Periodicaltest Mapeh10Bryan Mon RosaОценок пока нет
- National Congress of Veterinary Medicine Students-PowerpointДокумент33 страницыNational Congress of Veterinary Medicine Students-PowerpointbaruruydОценок пока нет
- Relevance of Biomarkers in SepsisДокумент51 страницаRelevance of Biomarkers in SepsisSANTOSH KUMAR BHASKARОценок пока нет
- NF6 Unit3Документ46 страницNF6 Unit3กิ่งกาญจน์ มูลโมกข์Оценок пока нет
- Value Proposition Apollo HospitalsДокумент2 страницыValue Proposition Apollo Hospitalsakashkr619Оценок пока нет
- Philo 3h NotesДокумент5 страницPhilo 3h Notesapi-3743951100% (3)
- IDA Membership FormДокумент3 страницыIDA Membership FormAbhijit LeleОценок пока нет
- Counselli NG in Hiv/Aids: Presented By-Bhawna Joshi Msc. N 2 Tear SNSRДокумент30 страницCounselli NG in Hiv/Aids: Presented By-Bhawna Joshi Msc. N 2 Tear SNSRBhawna JoshiОценок пока нет
- PV Lesson 1Документ242 страницыPV Lesson 1Ankita UpadhyayОценок пока нет
- Rite BlueprintДокумент11 страницRite BlueprintTal Lagura100% (1)
- PrincetonДокумент7 страницPrincetonangel nahdeeОценок пока нет
- Analisis Dukungan Suami Selama Kehamilan Terhadap Kunjungan Antenatal CareДокумент11 страницAnalisis Dukungan Suami Selama Kehamilan Terhadap Kunjungan Antenatal CarefirmianisaОценок пока нет