Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Post Traumatic Headache Disorder - 2020Документ26 страницPost Traumatic Headache Disorder - 2020Surat TanprawateОценок пока нет
- Status Epilepticus PathophysiologyДокумент22 страницыStatus Epilepticus PathophysiologySurat TanprawateОценок пока нет
- Headache Tutorial - Neuro Essential CMU2020Документ66 страницHeadache Tutorial - Neuro Essential CMU2020Surat Tanprawate100% (4)
- Neurological Examination - Pre-Med - 401Документ73 страницыNeurological Examination - Pre-Med - 401Surat Tanprawate100% (4)
- Headche:Dizzy Med Stud - 2016Документ51 страницаHeadche:Dizzy Med Stud - 2016Surat TanprawateОценок пока нет
- Status Epilepticus in Adult PDFДокумент22 страницыStatus Epilepticus in Adult PDFSurat TanprawateОценок пока нет
- New Era in Migraine Management - 2019 - HatYaiДокумент77 страницNew Era in Migraine Management - 2019 - HatYaiSurat Tanprawate100% (3)
- Neuro-Ophthalmology - Third Year Student - 2018Документ126 страницNeuro-Ophthalmology - Third Year Student - 2018Surat TanprawateОценок пока нет
- Migraine SubtypeДокумент55 страницMigraine SubtypeSurat Tanprawate100% (1)
- Headache Case Seminar - RCPTДокумент25 страницHeadache Case Seminar - RCPTSurat TanprawateОценок пока нет
- Headache Case Seminar - RCPTДокумент25 страницHeadache Case Seminar - RCPTSurat TanprawateОценок пока нет
- Refractory-Primary-Headache Surat PornchaiДокумент51 страницаRefractory-Primary-Headache Surat PornchaiSurat TanprawateОценок пока нет
- Headache in Emergency ConditionДокумент34 страницыHeadache in Emergency ConditionSurat TanprawateОценок пока нет
- Neuro Ophthalmology For Med Student - 2016Документ120 страницNeuro Ophthalmology For Med Student - 2016Surat Tanprawate100% (3)
- Basic Movement Disorder ApproachДокумент96 страницBasic Movement Disorder ApproachSurat Tanprawate100% (18)
- Acute Migraine Management, Chiangmai 2015Документ60 страницAcute Migraine Management, Chiangmai 2015Surat Tanprawate100% (1)
- Ambulatory Conference: Approach To Parkinson's DiseaseДокумент37 страницAmbulatory Conference: Approach To Parkinson's DiseaseSurat Tanprawate100% (1)
- DPP-4 Inhibitor and The BrainДокумент19 страницDPP-4 Inhibitor and The BrainSurat TanprawateОценок пока нет
- Physical Exam For DiagnosisДокумент61 страницаPhysical Exam For DiagnosisSurat Tanprawate100% (2)
- Physical Exam For DiagnosisДокумент61 страницаPhysical Exam For DiagnosisSurat Tanprawate100% (2)
- Resident Tutorial 57-Part 1Документ81 страницаResident Tutorial 57-Part 1Surat Tanprawate100% (1)
- Channelopathy of CNSДокумент55 страницChannelopathy of CNSSurat TanprawateОценок пока нет
- Neuro OphthalmologyДокумент114 страницNeuro OphthalmologySurat TanprawateОценок пока нет
- MS and NMO Update From ECTRIMS - Boston 2014 PDFДокумент43 страницыMS and NMO Update From ECTRIMS - Boston 2014 PDFSurat TanprawateОценок пока нет
- Headache You Should Know - SuratДокумент33 страницыHeadache You Should Know - SuratSurat Tanprawate100% (2)
- PD SubtypeДокумент11 страницPD SubtypeSurat TanprawateОценок пока нет
- Role AEDs in Migraine PreventionДокумент61 страницаRole AEDs in Migraine PreventionSurat TanprawateОценок пока нет
- MS and NMO Update From ECTRIMS - Boston 2014 PDFДокумент43 страницыMS and NMO Update From ECTRIMS - Boston 2014 PDFSurat TanprawateОценок пока нет
- Occam's Razor and Hickam's DictumДокумент6 страницOccam's Razor and Hickam's DictumSurat TanprawateОценок пока нет
- WN - jun14.BB M CohenДокумент12 страницWN - jun14.BB M CohenSurat TanprawateОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Merchant Shipping MINIMUM SAFE MANNING Regulations 2016Документ14 страницMerchant Shipping MINIMUM SAFE MANNING Regulations 2016Arthur SchoutОценок пока нет
- GSM Radio ConceptsДокумент3 страницыGSM Radio ConceptsMD SahidОценок пока нет
- Resolution: Owner/Operator, DocketedДокумент4 страницыResolution: Owner/Operator, DocketedDonna Grace Guyo100% (1)
- Amsterdam Pipe Museum - Snuff WorldwideДокумент1 страницаAmsterdam Pipe Museum - Snuff Worldwideevon1Оценок пока нет
- The Fluency Course Teacher Instructions PDFДокумент9 страницThe Fluency Course Teacher Instructions PDFGabriel da RochaОценок пока нет
- APRStt Implementation Notes PDFДокумент36 страницAPRStt Implementation Notes PDFCT2IWWОценок пока нет
- Cutler Hammer Dry Type TransformerДокумент220 страницCutler Hammer Dry Type TransformernprajanОценок пока нет
- Eco EssayДокумент3 страницыEco EssaymanthanОценок пока нет
- Final Matatag Epp Tle CG 2023 Grades 4 10Документ184 страницыFinal Matatag Epp Tle CG 2023 Grades 4 10DIVINE GRACE CABAHUGОценок пока нет
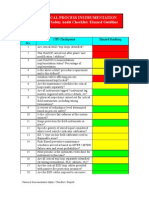
- Chemical Safety ChecklistДокумент3 страницыChemical Safety ChecklistPillai Sreejith100% (10)
- Asme b16.3 (1998) Malleable Iron Threaded FittingsДокумент30 страницAsme b16.3 (1998) Malleable Iron Threaded FittingsMarcos RosenbergОценок пока нет
- Material Safety Data Sheet: - AdsealДокумент12 страницMaterial Safety Data Sheet: - Adsealwuhan lalalaОценок пока нет
- British Birds 10 LondДокумент376 страницBritish Birds 10 Londcassy98Оценок пока нет
- BBO2020Документ41 страницаBBO2020qiuОценок пока нет
- Template Remarks For IIДокумент18 страницTemplate Remarks For IIjasleeneceОценок пока нет
- Model Contract FreelanceДокумент3 страницыModel Contract FreelancemarcosfreyervinnorskОценок пока нет
- Firing OrderДокумент5 страницFiring OrderCurtler PaquibotОценок пока нет
- Bankers ChoiceДокумент18 страницBankers ChoiceArchana ThirunagariОценок пока нет
- Data Structures and Algorithms SyllabusДокумент9 страницData Structures and Algorithms SyllabusBongbong GalloОценок пока нет
- Acronyms and AbbreviationsДокумент875 страницAcronyms and AbbreviationsLacky KrishnanОценок пока нет
- Intergard 475HS - Part B - EVA046 - GBR - ENG PDFДокумент10 страницIntergard 475HS - Part B - EVA046 - GBR - ENG PDFMohamed NouzerОценок пока нет
- QuerySurge Models Mappings DocumentДокумент28 страницQuerySurge Models Mappings Documentchiranjeev mishra100% (1)
- Shades Eq Gloss Large Shade ChartДокумент2 страницыShades Eq Gloss Large Shade ChartmeganОценок пока нет
- ENG 102 Essay PromptДокумент2 страницыENG 102 Essay Promptarshia winОценок пока нет
- Choosing An Effective Visual ToolДокумент9 страницChoosing An Effective Visual ToolAdil Bin KhalidОценок пока нет
- Automated Facilities Layout Past Present and FutureДокумент19 страницAutomated Facilities Layout Past Present and FutureJose Luis Diaz BetancourtОценок пока нет
- Unit: 1: Newton's Laws of Motion & Principle of Transmissibility of ForceДокумент5 страницUnit: 1: Newton's Laws of Motion & Principle of Transmissibility of ForceKunal SinghОценок пока нет
- A Sample Script For Public SpeakingДокумент2 страницыA Sample Script For Public Speakingalmasodi100% (2)
- Ultrasonic Based Distance Measurement SystemДокумент18 страницUltrasonic Based Distance Measurement SystemAman100% (2)
- Ioi Group - Capric Acid 98%Документ7 страницIoi Group - Capric Acid 98%Wong MjОценок пока нет