Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Tobacco Cessation PlanДокумент11 страницTobacco Cessation PlanEsteban García EcheverryОценок пока нет
- SCIT 1408 Applied Human Anatomy and Physiology II - Urinary System Chapter 25 BДокумент50 страницSCIT 1408 Applied Human Anatomy and Physiology II - Urinary System Chapter 25 BChuongОценок пока нет
- Bahasa InggrisДокумент6 страницBahasa InggrisSofi SusantoОценок пока нет
- The Effect of Tobacco Smoking Among Third Year Student Nurse in The University of LuzonДокумент6 страницThe Effect of Tobacco Smoking Among Third Year Student Nurse in The University of LuzonNeil Christian TadzОценок пока нет
- Complications of DiabetesДокумент3 страницыComplications of Diabetesa7wfОценок пока нет
- A Sonographic Sign of Moderate ToДокумент5 страницA Sonographic Sign of Moderate ToDivisi FER MalangОценок пока нет
- Pigeons: Animal SciencesДокумент15 страницPigeons: Animal SciencesSafi Ul RehmanОценок пока нет
- Nursing Management of HypertensionДокумент152 страницыNursing Management of HypertensionEnfermeriaAncam100% (3)
- Nowadays Young People Spend Too Much of Their Free Time in Shopping MallsДокумент3 страницыNowadays Young People Spend Too Much of Their Free Time in Shopping MallsYacine BenHmeidaОценок пока нет
- Abnormal Psychology Final Practice QuestionsДокумент16 страницAbnormal Psychology Final Practice QuestionsJames WilkesОценок пока нет
- What Is Malnutrition?: WastingДокумент6 страницWhat Is Malnutrition?: WastingĐoan VõОценок пока нет
- Is It True That GanodermaДокумент2 страницыIs It True That GanodermaRohit SharmaОценок пока нет
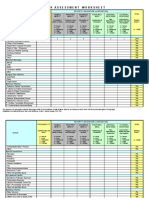
- IC Risk Assessment Worksheet - Kangas-V2.1-Aug.2010 1Документ4 страницыIC Risk Assessment Worksheet - Kangas-V2.1-Aug.2010 1Juon Vairzya AnggraeniОценок пока нет
- DSM OcdДокумент2 страницыDSM Ocdnmyza89Оценок пока нет
- GIEEE TGMP Policy Terms For 2022-23Документ5 страницGIEEE TGMP Policy Terms For 2022-23Janardhan Reddy TОценок пока нет
- Quiz 632 General Science For SSC ExaminationsДокумент4 страницыQuiz 632 General Science For SSC ExaminationsDibyendu SahuОценок пока нет
- A Comparative Clinical Evaluation of Eranda Taila Matra Basti With Combination of Mefenamic Acid and Dicyclomine in The Management of Udavartini W.S.R To Primary DysmenorrheaДокумент8 страницA Comparative Clinical Evaluation of Eranda Taila Matra Basti With Combination of Mefenamic Acid and Dicyclomine in The Management of Udavartini W.S.R To Primary DysmenorrheaEditor IJTSRDОценок пока нет
- Physiology of The Cell: H. Khorrami PH.DДокумент89 страницPhysiology of The Cell: H. Khorrami PH.Dkhorrami4Оценок пока нет
- Week 6 Nursing Care of The Family With Reproductive DisordersДокумент27 страницWeek 6 Nursing Care of The Family With Reproductive DisordersStefhanie Mae LazaroОценок пока нет
- Neurobiology of Sleep: Madhu Kalia4Документ5 страницNeurobiology of Sleep: Madhu Kalia4Julian ReyesОценок пока нет
- Conduction Blocks in Acute Myocardial Infarction: A Prospective StudyДокумент6 страницConduction Blocks in Acute Myocardial Infarction: A Prospective StudyJack JacksonОценок пока нет
- Celecoxib, Etoricoxib, DiclofenacДокумент13 страницCelecoxib, Etoricoxib, Diclofenacbaitur rohmahОценок пока нет
- ZFN, TALEN, and CRISPR-Cas-based Methods For Genome EngineeringДокумент9 страницZFN, TALEN, and CRISPR-Cas-based Methods For Genome EngineeringRomina Tamara Gil RamirezОценок пока нет
- Prioritization - FNCPДокумент10 страницPrioritization - FNCPJeffer Dancel67% (3)
- Resource Material - Day 1 Primary Register Activity - ANC Register - 0Документ3 страницыResource Material - Day 1 Primary Register Activity - ANC Register - 0Ranjeet Singh KatariaОценок пока нет
- 1 To 3Документ49 страниц1 To 3Vikki NandeshwarОценок пока нет
- CHCCCS015 Student Assessment Booklet Is (ID 97088) - FinalДокумент33 страницыCHCCCS015 Student Assessment Booklet Is (ID 97088) - FinalESRОценок пока нет
- Carbon Monoxide PoisoningДокумент31 страницаCarbon Monoxide PoisoningDheerajОценок пока нет
- Adult Failure To ThriveДокумент5 страницAdult Failure To Thriveasmika danaОценок пока нет
- Environmental Studies-FIRST UNIT-vkmДокумент59 страницEnvironmental Studies-FIRST UNIT-vkmRandomОценок пока нет