Вам также может понравиться
- CG en PDFДокумент335 страницCG en PDFJessicaPaolaGutiérrezAranaОценок пока нет
- 7 TH Semester Dermatology LecturesДокумент44 страницы7 TH Semester Dermatology LecturesChhabilal BastolaОценок пока нет
- Investigations For Thrombotic Tendencies - Australian Prescriber PDFДокумент6 страницInvestigations For Thrombotic Tendencies - Australian Prescriber PDFChhabilal BastolaОценок пока нет
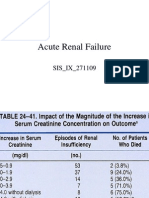
- Acute Renal FailureДокумент125 страницAcute Renal FailureChhabilal BastolaОценок пока нет
- Opioids in AnaesthesiaДокумент28 страницOpioids in AnaesthesiaChhabilal BastolaОценок пока нет
- Meningitis and Brain AbscessДокумент32 страницыMeningitis and Brain AbscessChhabilal BastolaОценок пока нет
- 7 TH Semester Anesthesia LecturesДокумент35 страниц7 TH Semester Anesthesia LecturesChhabilal BastolaОценок пока нет
- Oxygen TherapyДокумент44 страницыOxygen TherapyChhabilal BastolaОценок пока нет
- Altered Sensorium and Care of Unconscious PatientsДокумент17 страницAltered Sensorium and Care of Unconscious PatientsChhabilal BastolaОценок пока нет
- Unconscious PatientДокумент19 страницUnconscious PatientChhabilal BastolaОценок пока нет
- Dental Anatomy For MBBSДокумент33 страницыDental Anatomy For MBBSChhabilal BastolaОценок пока нет
- Emergency Drug Doses - PBS Doctor's Bag Items - Australian PrescriberДокумент4 страницыEmergency Drug Doses - PBS Doctor's Bag Items - Australian PrescriberChhabilal BastolaОценок пока нет
- ERC Guidelines 2005 Advanced Adult Life SupportДокумент48 страницERC Guidelines 2005 Advanced Adult Life SupportJoãoBrasil100% (2)
- ChronicKidneyDisease IX Semseter MBBSДокумент38 страницChronicKidneyDisease IX Semseter MBBSChhabilal BastolaОценок пока нет
- Kumj-Guideline For AuthorsДокумент6 страницKumj-Guideline For AuthorsChhabilal BastolaОценок пока нет
- Resusgl 2010Документ157 страницResusgl 2010Salman IslamОценок пока нет
- Snake Bite ManagementДокумент49 страницSnake Bite ManagementChhabilal BastolaОценок пока нет
- Usmle LabsДокумент3 страницыUsmle LabsAdnan KhurshidОценок пока нет
- Wellness and Fitness Exercise ManualДокумент63 страницыWellness and Fitness Exercise ManualcienciaxОценок пока нет
- How - To - Read - Guitar TabДокумент29 страницHow - To - Read - Guitar TabChhabilal Bastola100% (3)
- 2010 Step 2 CKДокумент76 страниц2010 Step 2 CKandres ord100% (2)
- 42 Deep Thought On Life, The Universe, and EverythingДокумент195 страниц42 Deep Thought On Life, The Universe, and EverythingHenry Ford100% (3)
- LyricsДокумент2 страницыLyricsChhabilal BastolaОценок пока нет
- Step 3: Content Description and General InformationДокумент73 страницыStep 3: Content Description and General Informations1234321Оценок пока нет
- Im Yours Chords: by Jason MrazДокумент2 страницыIm Yours Chords: by Jason MrazChhabilal BastolaОценок пока нет
- Top 100 QS World University Rankings For Medicine 2011 - Higher Education Network - Guardian ProfessionalДокумент5 страницTop 100 QS World University Rankings For Medicine 2011 - Higher Education Network - Guardian ProfessionalChhabilal BastolaОценок пока нет
- UsmleДокумент58 страницUsmleFaisal Chukwudera Adam100% (1)
- Lyrics and Chords From UltimateДокумент2 страницыLyrics and Chords From UltimateChhabilal BastolaОценок пока нет
- Top 100 QS World University Rankings For Medicine 2011 - Higher Education Network - Guardian ProfessionalДокумент5 страницTop 100 QS World University Rankings For Medicine 2011 - Higher Education Network - Guardian ProfessionalChhabilal BastolaОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Intraprocedural Imaging of Cardiovascular Interventions: Michael H. Picard Jonathan J. Passeri Jacob P. Dal-BiancoДокумент171 страницаIntraprocedural Imaging of Cardiovascular Interventions: Michael H. Picard Jonathan J. Passeri Jacob P. Dal-BiancoLina María CañónОценок пока нет
- Thromboembolic DisordersДокумент11 страницThromboembolic Disordersannu panchalОценок пока нет
- Australasian Emergency Nursing JournalДокумент7 страницAustralasian Emergency Nursing JournalPutriWulandariОценок пока нет
- European Heart Journal Supplements (2019) - SeptemberДокумент82 страницыEuropean Heart Journal Supplements (2019) - SeptemberBeard BeardОценок пока нет
- 1704-1702 CBAHI Common QuestionsДокумент32 страницы1704-1702 CBAHI Common Questionsshadi alshadafan100% (5)
- Clexane® 60mg/0.6ml SyringesДокумент8 страницClexane® 60mg/0.6ml Syringesnaga chaitanyaОценок пока нет
- National Safety Standards for HospitalsДокумент51 страницаNational Safety Standards for HospitalsAyman Ali100% (4)
- Physio 2.05 Bloodphysiology2 HemostasisДокумент9 страницPhysio 2.05 Bloodphysiology2 HemostasisSimon Peter Familara100% (1)
- Signal Assessment Report Embolic Thrombotic Events SMQ Covid 19 Vaccine Chadox1 S Recombinant Covid - enДокумент50 страницSignal Assessment Report Embolic Thrombotic Events SMQ Covid 19 Vaccine Chadox1 S Recombinant Covid - enFlorinelОценок пока нет
- Cardioversion of Atrial Fibrillation and AtrialДокумент13 страницCardioversion of Atrial Fibrillation and AtrialLabontu IustinaОценок пока нет
- Emboli ParuДокумент61 страницаEmboli ParuAndrew MakariosОценок пока нет
- Concept MapДокумент4 страницыConcept MapDud AccОценок пока нет
- Venous Thromboembolic Diseases: Deep Vein Thrombosis: Support For Education and Learning Clinical Case ScenariosДокумент64 страницыVenous Thromboembolic Diseases: Deep Vein Thrombosis: Support For Education and Learning Clinical Case ScenariosNabila TyaОценок пока нет
- Practical Guide To Casting: Author: Matthew Pitt Senior Orthopaedic PractitionerДокумент31 страницаPractical Guide To Casting: Author: Matthew Pitt Senior Orthopaedic Practitionerbinod rijalОценок пока нет
- Embolism: Types, Causes, PathophysiologyДокумент13 страницEmbolism: Types, Causes, PathophysiologySandeep Bansal100% (1)
- COVID 19 Is A Systemic Vascular HemopathyДокумент34 страницыCOVID 19 Is A Systemic Vascular HemopathyYuri YogyaОценок пока нет
- VTE Report FormДокумент4 страницыVTE Report FormHosam GomaaОценок пока нет
- Cerazette®: What Is in This LeafletДокумент9 страницCerazette®: What Is in This LeafletAce PedrosoОценок пока нет
- NCM 118Документ7 страницNCM 118Hazel MiraranОценок пока нет
- 08 DN 005 BA Int OkДокумент64 страницы08 DN 005 BA Int OkvbogachevОценок пока нет
- Preanesthesia Evaluation For Noncardiac Surgery - UpToDate PDFДокумент86 страницPreanesthesia Evaluation For Noncardiac Surgery - UpToDate PDFCharlie Bellow100% (1)
- 4 - Post Operative Nursing ManagementДокумент38 страниц4 - Post Operative Nursing ManagementraghadОценок пока нет
- Warfarin ManagementДокумент104 страницыWarfarin ManagementMr XОценок пока нет
- Pub Assign 1Документ7 страницPub Assign 1Areesha KaleemОценок пока нет
- WARFARIN Prescribing Guidelines For The Management of Patients On Anticoagulant Therapy WIRRAL NHSДокумент14 страницWARFARIN Prescribing Guidelines For The Management of Patients On Anticoagulant Therapy WIRRAL NHSNavojit ChowdhuryОценок пока нет
- Managing FP Side Effects and Complications: Prepared by Tsiyon. K Jimma Ethiopia JULY 2021Документ59 страницManaging FP Side Effects and Complications: Prepared by Tsiyon. K Jimma Ethiopia JULY 2021Yonas AbebeОценок пока нет
- Choosing the Right Birth Control Pill for TeensДокумент16 страницChoosing the Right Birth Control Pill for TeensrakhelmaharanipybОценок пока нет
- Clinical manifestations of inflammatory bowel disease in childrenДокумент926 страницClinical manifestations of inflammatory bowel disease in childrenFlorin Calin LungОценок пока нет
- Sulodexide For The Prevention of Recurrent Venous ThromboembolismДокумент40 страницSulodexide For The Prevention of Recurrent Venous ThromboembolismMELVINОценок пока нет
- General Surgery Exam Syllabus BlueprintДокумент59 страницGeneral Surgery Exam Syllabus BlueprintSamiaNazОценок пока нет