Вам также может понравиться
- Unit 04 - Pharmacology of Endocrine System With AnswerДокумент3 страницыUnit 04 - Pharmacology of Endocrine System With Answersadia parveen100% (1)
- Calculus Cheat Sheet Limits Definitions Limit at InfinityДокумент11 страницCalculus Cheat Sheet Limits Definitions Limit at Infinityapi-1192241886% (7)
- Nov 2017 Infantile Spasms WebinarДокумент22 страницыNov 2017 Infantile Spasms WebinartetiОценок пока нет
- Well-Being Behind BarsДокумент55 страницWell-Being Behind BarsAtty. Jana Felice Gonzalez100% (1)
- ANTECEDENTS and CONSEQUENCESДокумент3 страницыANTECEDENTS and CONSEQUENCESYroen Faith D. TalonОценок пока нет
- Thyroid Disorders in PregnancyДокумент46 страницThyroid Disorders in PregnancyMara Medina - BorleoОценок пока нет
- Columnar Insulin Dosing Chart : (1 ML 1 Unit)Документ1 страницаColumnar Insulin Dosing Chart : (1 ML 1 Unit)Philippe KinnaerОценок пока нет
- Hypothyroidism Lesson PlanДокумент20 страницHypothyroidism Lesson PlanDimpal Choudhary50% (2)
- Neuroscience - 4.3 - Examination of Cerebellar Systems and Meninges (KSD)Документ4 страницыNeuroscience - 4.3 - Examination of Cerebellar Systems and Meninges (KSD)Kevin C. AguilarОценок пока нет
- What Is HypothalamusДокумент15 страницWhat Is HypothalamusyogieОценок пока нет
- Fmri and PsychologyДокумент14 страницFmri and Psychologyapi-478952871Оценок пока нет
- Family Communication - JiaДокумент6 страницFamily Communication - JiaRey Belano TacsayОценок пока нет
- Peripheral Nervous System WordДокумент4 страницыPeripheral Nervous System WordJesi QuiambaoОценок пока нет
- Anatomy of Hypothalamus and HypophysisДокумент3 страницыAnatomy of Hypothalamus and HypophysisshindyОценок пока нет
- Movement Disorders BabcockДокумент19 страницMovement Disorders BabcockBaiq Trisna SatrianaОценок пока нет
- Inflammatory ResponseДокумент7 страницInflammatory Responseᵇᵅᵇᵞ Anden GonzagaОценок пока нет
- Disoreder of PerceptionДокумент36 страницDisoreder of PerceptionUmar Khan100% (1)
- AntidepresentДокумент34 страницыAntidepresentmariaОценок пока нет
- Case History M.SCДокумент10 страницCase History M.SCRaksha RNОценок пока нет
- Types of ParalysisДокумент6 страницTypes of ParalysisLoh Wei ChiehОценок пока нет
- Growth and Development: Infancy Early Childhood Middle Childhood AdolescentДокумент42 страницыGrowth and Development: Infancy Early Childhood Middle Childhood AdolescentJohn Ervin AgenaОценок пока нет
- Internal Ear: Labyrinth (Figure 23-21) - The Membranous Labyrinth Is Derived From An EctodermalДокумент7 страницInternal Ear: Labyrinth (Figure 23-21) - The Membranous Labyrinth Is Derived From An EctodermalmohamadОценок пока нет
- Psychology SchizopherniaДокумент21 страницаPsychology SchizopherniaDevesh SaiОценок пока нет
- The Detailed Neurologic Examination in Adults - UpToDate PDFДокумент29 страницThe Detailed Neurologic Examination in Adults - UpToDate PDFMiguel GarciaОценок пока нет
- Health, Stress, and CopingДокумент43 страницыHealth, Stress, and CopingKar Gayee100% (1)
- The Brain Stem: Location and Basic PhysiologyДокумент33 страницыThe Brain Stem: Location and Basic PhysiologyMohammad AliОценок пока нет
- Ap Psychology Chapter 17 OutlineДокумент6 страницAp Psychology Chapter 17 Outlineccarroll2722100% (1)
- Receptor PhysiologyДокумент34 страницыReceptor PhysiologyKarl Torres Uganiza RmtОценок пока нет
- Serotonin Dopamine and NeurotransmittersДокумент6 страницSerotonin Dopamine and Neurotransmittersapi-533834366Оценок пока нет
- The Central Nervous System: BrainДокумент12 страницThe Central Nervous System: BrainsheinelleОценок пока нет
- Diseases of The Central Nervous SystemДокумент5 страницDiseases of The Central Nervous Systemlady_angelzОценок пока нет
- Hand Outs Oncologic Brain DsoДокумент9 страницHand Outs Oncologic Brain DsoJessa AdenigОценок пока нет
- Infant ReflexesДокумент1 страницаInfant ReflexesJohn Dela VegaОценок пока нет
- Neurodevelopmental DisordersДокумент33 страницыNeurodevelopmental DisordersBrett de GuzmanОценок пока нет
- Dysphagia Due To Upper Esophageal Sphincter DisordДокумент3 страницыDysphagia Due To Upper Esophageal Sphincter DisordEustakia Rini Kartika DewiОценок пока нет
- Defense Mechanism: Drvksahu Resident PsychiatryДокумент74 страницыDefense Mechanism: Drvksahu Resident PsychiatryMudassar HussainОценок пока нет
- Neurologic ExaminationДокумент67 страницNeurologic Examinationሀይደር ዶ.ር100% (1)
- What Is AutismДокумент2 страницыWhat Is AutismTimothy Teh Ewe TimОценок пока нет
- Reflex ExamДокумент4 страницыReflex ExamDan Ali100% (1)
- Homeostasis and Feedback Loops AjarДокумент34 страницыHomeostasis and Feedback Loops AjarPutri Sari SeptirianiОценок пока нет
- Developmental Stage of ChildhoodДокумент31 страницаDevelopmental Stage of ChildhoodIrisFierSaewelОценок пока нет
- Cerebral Malaria (CM) Prof. WBP Matuja, MuhasДокумент20 страницCerebral Malaria (CM) Prof. WBP Matuja, MuhasAnonymous TCZf45C10Оценок пока нет
- Psychiatric Disorders During Pregnancy and BirthДокумент39 страницPsychiatric Disorders During Pregnancy and Birthvictor onapaОценок пока нет
- ADHD PowerpointДокумент17 страницADHD PowerpointArlyn CastroОценок пока нет
- Basal GangliaДокумент6 страницBasal Ganglia381a53c99bОценок пока нет
- Developmental Dysplasia of The Hip - Clinical Features and Diagnosis - UpToDateДокумент13 страницDevelopmental Dysplasia of The Hip - Clinical Features and Diagnosis - UpToDateFernandoVianaОценок пока нет
- Human Development: Management Public Behaviour Novita D PutriДокумент68 страницHuman Development: Management Public Behaviour Novita D PutriNovi JCorpsОценок пока нет
- Asdv 2Документ51 страницаAsdv 2api-434818140Оценок пока нет
- The Human Nervous Syste1Документ10 страницThe Human Nervous Syste1taytay321Оценок пока нет
- What Reflexes Should Be Present in A Newborn?Документ4 страницыWhat Reflexes Should Be Present in A Newborn?Nicole OrtizОценок пока нет
- Sensory Integration y AДокумент4 страницыSensory Integration y ASuperfixenОценок пока нет
- Chart. Piaget's 4 Stages of Cognitive DevelopmentДокумент3 страницыChart. Piaget's 4 Stages of Cognitive DevelopmentJULIA ESTEFANIA ALFARO HURTADOОценок пока нет
- REFLEXESДокумент15 страницREFLEXESSonali Soumyashree100% (2)
- Electroconvulsive TherapyДокумент4 страницыElectroconvulsive TherapyGabi CeriaОценок пока нет
- NeuronsДокумент18 страницNeuronsErica Mae MejiaОценок пока нет
- The Neurorelational Framework Final 9.25.13 PDFДокумент5 страницThe Neurorelational Framework Final 9.25.13 PDFEmi MedinaОценок пока нет
- Trendelenburg Test:: Hip Special TestsДокумент3 страницыTrendelenburg Test:: Hip Special TestsIulia ElenaОценок пока нет
- Neurotransmitters in Schizophrenia: Dr. Adel El SheshaiДокумент47 страницNeurotransmitters in Schizophrenia: Dr. Adel El SheshaielvinegunawanОценок пока нет
- Neural Basis of MemoryДокумент9 страницNeural Basis of Memoryapi-219687122Оценок пока нет
- Identification and Diagnosis: Compulsive Alcoholic BeveragesДокумент3 страницыIdentification and Diagnosis: Compulsive Alcoholic BeveragesKaren JulaoОценок пока нет
- Mental Status Examination (Mse) : The MSE Is A "Snapshot" of A Patient at A Specific TimeДокумент19 страницMental Status Examination (Mse) : The MSE Is A "Snapshot" of A Patient at A Specific TimeSree ZОценок пока нет
- Temporal LobeДокумент68 страницTemporal LobeRupinder GillОценок пока нет
- Counselling BCДокумент28 страницCounselling BCAPOORVA PANDEYОценок пока нет
- Cerebral PalsyДокумент3 страницыCerebral PalsyBrent NicholsОценок пока нет
- Summary of Tara Delaney's 101 Games and Activities for Children With Autism, Asperger’s and Sensory Processing DisordersОт EverandSummary of Tara Delaney's 101 Games and Activities for Children With Autism, Asperger’s and Sensory Processing DisordersОценок пока нет
- Mirtazapine PDF PDFДокумент23 страницыMirtazapine PDF PDFBoneGrissleОценок пока нет
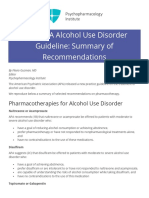
- 2018 APA Alcohol Use Disorder Guideline: Summary of RecommendationsДокумент3 страницы2018 APA Alcohol Use Disorder Guideline: Summary of RecommendationsBoneGrissleОценок пока нет
- Experimental Verification of Snell's Law: Equipment ListДокумент3 страницыExperimental Verification of Snell's Law: Equipment Listbdevlin822Оценок пока нет
- Particle PhysicsДокумент16 страницParticle PhysicsBoneGrissleОценок пока нет
- Luteinizing and Follicle Stimulating Hormone (Powerpoint)Документ23 страницыLuteinizing and Follicle Stimulating Hormone (Powerpoint)Phoebe Guevarra100% (6)
- Pituitary DisordersДокумент38 страницPituitary DisordersJaspreet KangОценок пока нет
- MedicinaДокумент73 страницыMedicinachubura_je_raj100% (1)
- Clinical Scoring Scales in ThyroidologyДокумент16 страницClinical Scoring Scales in ThyroidologyafadurОценок пока нет
- Journal Diabetes MellitusДокумент11 страницJournal Diabetes Mellitusnabila noorОценок пока нет
- Random Blood Sugar Estimation and Its SignificanceДокумент11 страницRandom Blood Sugar Estimation and Its Significanceapi-38237850% (1)
- Jurnal 1Документ7 страницJurnal 1Sri Wahyuni NawawiОценок пока нет
- DiabetesДокумент1 страницаDiabetesapi-444202349Оценок пока нет
- Gestational Diabetes MellitusДокумент31 страницаGestational Diabetes MellitusJasmine PraveenОценок пока нет
- Chemical Pathology Job Description December 2011Документ9 страницChemical Pathology Job Description December 2011Chengyuan ZhangОценок пока нет
- Pituitary Gland: The Hormones and Their Function Presented By: Gufran Bulbul Rono Ciit IslamabadДокумент16 страницPituitary Gland: The Hormones and Their Function Presented By: Gufran Bulbul Rono Ciit IslamabadGufran Gb RonoОценок пока нет
- Endocrine System NotesДокумент14 страницEndocrine System NotesSteven100% (1)
- Insulin ResistanceДокумент48 страницInsulin ResistanceLavina JainОценок пока нет
- Pubertad TempranaДокумент10 страницPubertad TempranaLiz Valentina Jordan MoyaОценок пока нет
- Analysing The Levels of Various Biochemical Markers (T3, T4, and TSH) in Iraqi Patients With Thyroid ProblemsДокумент10 страницAnalysing The Levels of Various Biochemical Markers (T3, T4, and TSH) in Iraqi Patients With Thyroid ProblemsCentral Asian StudiesОценок пока нет
- Testing During Pregnancy: David G. Grenache, PHD University of Utah & Arup Laboratories Salt Lake City, UtДокумент54 страницыTesting During Pregnancy: David G. Grenache, PHD University of Utah & Arup Laboratories Salt Lake City, Utمحمد عمران راناОценок пока нет
- Endocrine System QuizДокумент1 страницаEndocrine System Quizapi-368213959Оценок пока нет
- The Endocrine SystemДокумент18 страницThe Endocrine SystemPhea VillarealОценок пока нет
- Testosterone Replacement Therapy, A Recipe For Success - John Crisler, D.O.Документ8 страницTestosterone Replacement Therapy, A Recipe For Success - John Crisler, D.O.gstrohlОценок пока нет
- Quiz EndocrineДокумент16 страницQuiz EndocrineMon DoceОценок пока нет
- Pharm Exam 4 ReviewДокумент2 страницыPharm Exam 4 ReviewHwi GNDCОценок пока нет
- DIABETES MELLITUS - DR Neelakanta KaradkalДокумент45 страницDIABETES MELLITUS - DR Neelakanta KaradkalNRK A OFFICIALОценок пока нет
- General Medicine Lec4 Adrenal GlandsДокумент9 страницGeneral Medicine Lec4 Adrenal GlandsAli MOОценок пока нет
- DynaMed Plus - Thyroid NoduleДокумент85 страницDynaMed Plus - Thyroid NoduleGamer MadaОценок пока нет
- Investigatory Project ON Diabetes Mellitus: Name: Sagnik KulaviДокумент22 страницыInvestigatory Project ON Diabetes Mellitus: Name: Sagnik Kulavisancharini kulaviОценок пока нет
- PhysioEx Exercise 4 Activity 3Документ3 страницыPhysioEx Exercise 4 Activity 3PabloAndresPalaciosAgilaОценок пока нет