Вам также может понравиться
- MATH8-Relations and Functions Worksheet AnswersДокумент15 страницMATH8-Relations and Functions Worksheet AnswersRhealyn Joy Narciso100% (2)
- Chapter 12 Drugs and The Autonomic Nervous System PDFДокумент10 страницChapter 12 Drugs and The Autonomic Nervous System PDFMaha KhanОценок пока нет
- Personality Drawing TestДокумент1 страницаPersonality Drawing TestVanessa SantosОценок пока нет
- Critical Care Calculations Study GuideДокумент6 страницCritical Care Calculations Study GuideAja Blue100% (2)
- Personality Drawing TestДокумент1 страницаPersonality Drawing TestVanessa SantosОценок пока нет
- Stone LowOxalateDiet PDFДокумент7 страницStone LowOxalateDiet PDFVanessa Santos0% (1)
- Versant ModifiedДокумент57 страницVersant ModifiedAryan Kharadkar100% (3)
- Adrenergic Receptors 2Документ2 страницыAdrenergic Receptors 2Mirumbi Kefa MomanyiОценок пока нет
- Epinephrine Sympthomimic AdrenergicДокумент19 страницEpinephrine Sympthomimic AdrenergicAlee Iz HarОценок пока нет
- SY - Medichem i -Drugs acting on ANS (1)Документ83 страницыSY - Medichem i -Drugs acting on ANS (1)KevalОценок пока нет
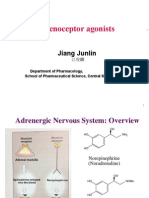
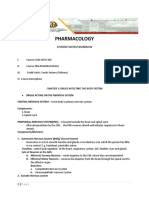
- I. Adrenergic Nervous System: OverviewДокумент71 страницаI. Adrenergic Nervous System: OverviewPravita BalijepalliОценок пока нет
- Assignment On Adrenergic ReceptorДокумент13 страницAssignment On Adrenergic ReceptoryannaingОценок пока нет
- Physiology of Adrenergic ReceptorsДокумент3 страницыPhysiology of Adrenergic ReceptorsShailendra YadavОценок пока нет
- L9 Sympathomimetics Lytics REVISED 2017 PDFДокумент49 страницL9 Sympathomimetics Lytics REVISED 2017 PDFVea AngelesОценок пока нет
- Inotropic Agents: Submitted ToДокумент87 страницInotropic Agents: Submitted Toraman kumariОценок пока нет
- Adrenergic DrugsДокумент21 страницаAdrenergic DrugsArturo RinconОценок пока нет
- IntroductIon To AutonomousДокумент29 страницIntroductIon To AutonomousMerve kdkkОценок пока нет
- Adrenergic Agents PharmacologyДокумент6 страницAdrenergic Agents PharmacologyMohamed OmerОценок пока нет
- I. Adrenergic Nervous System: OverviewДокумент71 страницаI. Adrenergic Nervous System: Overviewأمجد محمدОценок пока нет
- Adrenergic Drugs IДокумент3 страницыAdrenergic Drugs IMirumbi Kefa MomanyiОценок пока нет
- L17 - Adrenergics IIДокумент6 страницL17 - Adrenergics IIyasaira707Оценок пока нет
- Pharma Mod 11Документ12 страницPharma Mod 11ANGELA SHANE AGUSTINОценок пока нет
- Mohammad Ryad Goulvaden 5 Year Faculty of PharmacyДокумент46 страницMohammad Ryad Goulvaden 5 Year Faculty of PharmacypharmryadОценок пока нет
- Kee: Pharmacology, 8th Edition: Chapter 18: Adrenergic Agonists and Adrenergic Blockers Downloadable Key PointsДокумент2 страницыKee: Pharmacology, 8th Edition: Chapter 18: Adrenergic Agonists and Adrenergic Blockers Downloadable Key PointsLondera BainОценок пока нет
- ANS ReceptorsДокумент14 страницANS ReceptorsAisha AliОценок пока нет
- Case Study 1&2 - Group ActivityДокумент2 страницыCase Study 1&2 - Group ActivityChesca LayosaОценок пока нет
- Adrenoceptor Agonist and Antagonist Drugs-2014.10.7pptДокумент83 страницыAdrenoceptor Agonist and Antagonist Drugs-2014.10.7pptking_gold100% (1)
- Phl211 Sns 14th Lecture SFДокумент10 страницPhl211 Sns 14th Lecture SFALNAKIОценок пока нет
- SympathomimeticДокумент56 страницSympathomimeticvarish0% (1)
- Pharmacology: Students Notes/ WorkbookДокумент50 страницPharmacology: Students Notes/ WorkbookPABLO, JACKSON P.Оценок пока нет
- Adrenergic & Antiadrenergic DrugsДокумент54 страницыAdrenergic & Antiadrenergic DrugsUzma KhanОценок пока нет
- By: Professor Emiliano Z. Sison JRДокумент40 страницBy: Professor Emiliano Z. Sison JRT Z BenОценок пока нет
- PharmaДокумент27 страницPharmaapi-19916399Оценок пока нет
- Pharm ANSДокумент45 страницPharm ANSaditya_goel_10Оценок пока нет
- Adrenergic Receptors GuideДокумент3 страницыAdrenergic Receptors GuideAhmad Ikbal PurnawarmanОценок пока нет
- Adrenergic AgentsДокумент57 страницAdrenergic AgentsAn Lo100% (1)
- PharmacologyДокумент236 страницPharmacologynbde2100% (5)
- Subject: Pharmacology Topic: ANS 2 Lecturer: Maria Luisa D. Delacruz, M.D. Date of Lecture:August 3, 2011 Transcriptionist: Anonymous Pages: 16Документ16 страницSubject: Pharmacology Topic: ANS 2 Lecturer: Maria Luisa D. Delacruz, M.D. Date of Lecture:August 3, 2011 Transcriptionist: Anonymous Pages: 16dtimtimanОценок пока нет
- Adrenergic Agonists and AntagonistsДокумент9 страницAdrenergic Agonists and Antagonistsstephanienwafor18Оценок пока нет
- Norepinephrine - Released From Postganglionic: Autonomic Nervous System MedicationsДокумент7 страницNorepinephrine - Released From Postganglionic: Autonomic Nervous System MedicationsJohn denver FloresОценок пока нет
- DBMS Notes - Module 02 Section 02 Sympathetic Nervous SystemДокумент11 страницDBMS Notes - Module 02 Section 02 Sympathetic Nervous SystemSaeidreza SardariОценок пока нет
- Autonomic Nervous System: Dr. Ahmed Elfatih Ahmed Clinical PharmacologistДокумент25 страницAutonomic Nervous System: Dr. Ahmed Elfatih Ahmed Clinical Pharmacologistكسلان اكتب اسميОценок пока нет
- Specific MedicationsДокумент10 страницSpecific MedicationsMico Adrian Depositario Dema-alaОценок пока нет
- Second Seminar Discussion On ANS PharmacologyДокумент21 страницаSecond Seminar Discussion On ANS PharmacologyDavid lufafaОценок пока нет
- Adrenergic& Antiadrengeic DrugsДокумент39 страницAdrenergic& Antiadrengeic DrugsAsif Ali LashariОценок пока нет
- NeurotransmittersДокумент21 страницаNeurotransmittersYannie GomezОценок пока нет
- 41.5A: Epinephrine and Norepinephrine: Key PointsДокумент2 страницы41.5A: Epinephrine and Norepinephrine: Key PointsAshley MudzingwaОценок пока нет
- Lesson 3Документ27 страницLesson 3Dipika Rani sahuОценок пока нет
- Sympathomimetics (Catecholamines & Non Catecholamines)Документ99 страницSympathomimetics (Catecholamines & Non Catecholamines)Raheel JavaidОценок пока нет
- Adrenergic PharmacologyДокумент17 страницAdrenergic PharmacologyCatОценок пока нет
- Adrenergic Agonists Lecture 1 - ClarkДокумент49 страницAdrenergic Agonists Lecture 1 - ClarkHaileris1Оценок пока нет
- Chemical Transmission in the Synapse: Neurotransmitters and ReceptorsДокумент24 страницыChemical Transmission in the Synapse: Neurotransmitters and ReceptorslibreizanОценок пока нет
- SympathomimeticsДокумент25 страницSympathomimeticsMirza Shaharyar BaigОценок пока нет
- Intro To Pharmacology Study GuideДокумент93 страницыIntro To Pharmacology Study GuideMichelle Morgan LongstrethОценок пока нет
- Reviewer of A PsychologyДокумент55 страницReviewer of A PsychologyCAMMILLE EDZ FERRAS SELONGОценок пока нет
- Autonomic Nervous System AgentsДокумент14 страницAutonomic Nervous System AgentsRhenier S. Ilado100% (1)
- Autonomic Nervous System - MidtermДокумент35 страницAutonomic Nervous System - MidtermHeizmaebrizОценок пока нет
- Pharma Script 5Документ12 страницPharma Script 5Hashim GhazoОценок пока нет
- ANS PharmacologyДокумент24 страницыANS PharmacologySOMOSCOОценок пока нет
- Pharmacology Module For FinalsДокумент11 страницPharmacology Module For FinalsCarlo GaradoОценок пока нет
- Sympathomimetics and SympatholyticsДокумент3 страницыSympathomimetics and Sympatholyticsbunso padillaОценок пока нет
- Cathecolamine, Sympathomimetic DrugsДокумент24 страницыCathecolamine, Sympathomimetic DrugsEric AryantoОценок пока нет
- Chicken Mole EnchiladasДокумент2 страницыChicken Mole EnchiladasVanessa SantosОценок пока нет
- Characteristics of Greek LiteratureДокумент2 страницыCharacteristics of Greek LiteratureVanessa Santos100% (2)
- Asian Recipes - Dessert Delights (With I - Ho, CharlesДокумент154 страницыAsian Recipes - Dessert Delights (With I - Ho, CharlesVanessa Santos100% (4)
- Chicken and Rice: IngredientsДокумент1 страницаChicken and Rice: IngredientsVanessa SantosОценок пока нет
- Acute Abdominal Pain and Acute AppendicitisДокумент8 страницAcute Abdominal Pain and Acute AppendicitisdrtpkОценок пока нет
- Copar Final3Документ4 страницыCopar Final3Vanessa SantosОценок пока нет
- Ps Calc GuideДокумент30 страницPs Calc GuideMzee321Оценок пока нет
- Philippine Constitution PDFДокумент53 страницыPhilippine Constitution PDFVanessa SantosОценок пока нет
- A Spark of ExistenceДокумент16 страницA Spark of ExistenceVanessa SantosОценок пока нет
- The CourtДокумент6 страницThe CourtVanessa SantosОценок пока нет
- Y Study CalculusДокумент5 страницY Study CalculusVanessa SantosОценок пока нет
- Marble speed needed to loop without fallingДокумент1 страницаMarble speed needed to loop without fallingVanessa SantosОценок пока нет
- Common Communicable DiseasesДокумент213 страницCommon Communicable Diseasesɹǝʍdןnos100% (24)
- 40 Items Comprehensive NCLEX ReviewДокумент20 страниц40 Items Comprehensive NCLEX Reviewclumsy16Оценок пока нет
- IMCIДокумент57 страницIMCIwyndzОценок пока нет
- LymphomaДокумент15 страницLymphomaVanessa SantosОценок пока нет
- Spinal Disc HerniationДокумент12 страницSpinal Disc HerniationVanessa SantosОценок пока нет
- Republic Act No 9173Документ5 страницRepublic Act No 9173Vanessa SantosОценок пока нет
- Shock Case Presentation: General DataДокумент1 страницаShock Case Presentation: General DataVanessa SantosОценок пока нет
- GreekДокумент7 страницGreekVanessa SantosОценок пока нет
- FractureДокумент58 страницFractureVanessa SantosОценок пока нет
- IMCIДокумент57 страницIMCIwyndzОценок пока нет
- AgingДокумент9 страницAgingVanessa SantosОценок пока нет
- CDPДокумент9 страницCDPVanessa SantosОценок пока нет
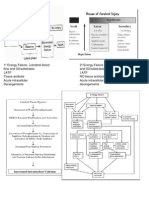
- 1º Energy FailureДокумент1 страница1º Energy FailureVanessa SantosОценок пока нет
- Sundar KandvalmikiДокумент98 страницSundar Kandvalmikifactree09Оценок пока нет
- GMsetДокумент8 страницGMsetdilo001Оценок пока нет
- Datta Das FET ExplanationДокумент2 страницыDatta Das FET ExplanationJulie HaydenОценок пока нет
- Ampersand MenuДокумент5 страницAmpersand MenuJozefОценок пока нет
- Print Date:: Container No NO Size Seal No Seal Party Supplier Status Movement TypeДокумент3 страницыPrint Date:: Container No NO Size Seal No Seal Party Supplier Status Movement TypeYudha PermanaОценок пока нет
- Principle Harmony RhythmДокумент16 страницPrinciple Harmony RhythmRosalinda PanopioОценок пока нет
- Overlord - Volume 01 - The Undead KingДокумент223 страницыOverlord - Volume 01 - The Undead KingPaulo FordheinzОценок пока нет
- Screenshot 2023-01-03 at 9.25.34 AM PDFДокумент109 страницScreenshot 2023-01-03 at 9.25.34 AM PDFAzri ZakwanОценок пока нет
- QUESTION A2 and A3 Examples PDFДокумент24 страницыQUESTION A2 and A3 Examples PDFDemian VeОценок пока нет
- Vishwabhanu Oct '18 - Jan '19Документ26 страницVishwabhanu Oct '18 - Jan '19vedicvision99100% (3)
- Tec Relay 52GДокумент3 страницыTec Relay 52Gimmer nainggolanОценок пока нет
- Director's Report Highlights Record Wheat Production in IndiaДокумент80 страницDirector's Report Highlights Record Wheat Production in Indiakamlesh tiwariОценок пока нет
- Diagram "From-To" Pada Optimasi Tata Letak Berorientasi Proses (Process Layout)Документ17 страницDiagram "From-To" Pada Optimasi Tata Letak Berorientasi Proses (Process Layout)Febrian Satrio WicaksonoОценок пока нет
- Mitchella Partridge Berry Materia Medica HerbsДокумент3 страницыMitchella Partridge Berry Materia Medica HerbsAlejandra GuerreroОценок пока нет
- II Unit - End EffectorsДокумент49 страницII Unit - End EffectorsGnanasekarОценок пока нет
- Art-App-Module-12 Soulmaking, Improvisation, Installation, & TranscreationДокумент4 страницыArt-App-Module-12 Soulmaking, Improvisation, Installation, & TranscreationJohn Mark D. RoaОценок пока нет
- Textile Pretreatment and Finishing 2023Документ205 страницTextile Pretreatment and Finishing 2023Aweru gebremariamОценок пока нет
- Instruction Manual: E2M40 and E2M80 Rotary Vacuum PumpsДокумент46 страницInstruction Manual: E2M40 and E2M80 Rotary Vacuum PumpsVicki NugrohoОценок пока нет
- Module 37 Nur 145Документ38 страницModule 37 Nur 145Marga WreatheОценок пока нет
- Design of PID controllersДокумент4 страницыDesign of PID controllersFseha GetahunОценок пока нет
- Com Statement (HT APFC22 - 02)Документ2 страницыCom Statement (HT APFC22 - 02)SOUMENОценок пока нет
- Patient Positioning: Complete Guide For Nurses: Marjo S. Malabanan, R.N.,M.NДокумент43 страницыPatient Positioning: Complete Guide For Nurses: Marjo S. Malabanan, R.N.,M.NMercy Anne EcatОценок пока нет
- Contact GRRSB Team for InquiriesДокумент2 страницыContact GRRSB Team for Inquiriesmsis81Оценок пока нет
- How Does Marijuana Affect The BrainДокумент3 страницыHow Does Marijuana Affect The BrainWanNurAtikahОценок пока нет
- Presentation 123Документ13 страницPresentation 123Harishitha ManivannanОценок пока нет
- Ericsson Microwave Outlook 2021Документ16 страницEricsson Microwave Outlook 2021Ahmed HussainОценок пока нет
- Aubrey Debut ScriptДокумент5 страницAubrey Debut ScriptKevin Jones CalumpangОценок пока нет
- Pemanfaatan Limbah Spanduk Plastik (Flexy Banner) Menjadi Produk Dekorasi RuanganДокумент6 страницPemanfaatan Limbah Spanduk Plastik (Flexy Banner) Menjadi Produk Dekorasi RuanganErvan Maulana IlyasОценок пока нет