Вам также может понравиться
- Application 9-10 NewДокумент4 страницыApplication 9-10 NewTemple Beth SholomОценок пока нет
- Admin ApplicationДокумент3 страницыAdmin ApplicationRedeemer Lutheran SchoolОценок пока нет
- Student Personal Info SheetДокумент5 страницStudent Personal Info SheetAhmad Rash SarabiОценок пока нет
- Notes: Face AmountДокумент4 страницыNotes: Face Amountqris24Оценок пока нет
- If You Need More Space Use An Extra PageДокумент3 страницыIf You Need More Space Use An Extra PageMohammed Sabeel KinggОценок пока нет
- Formulir Isian UsaДокумент5 страницFormulir Isian UsaFika FebrianaОценок пока нет
- GAL Application - Become A GAL in SCДокумент5 страницGAL Application - Become A GAL in SCWylde FaerieОценок пока нет
- Student Profile Form 1Документ1 страницаStudent Profile Form 1Angelika KlaireОценок пока нет
- Sis-Form SLNHSДокумент1 страницаSis-Form SLNHSMICHAEL RUELOОценок пока нет
- CTW Teacher Volunteer FormДокумент3 страницыCTW Teacher Volunteer FormAllanОценок пока нет
- Parent/Guardian Information: Continued On ReverseДокумент2 страницыParent/Guardian Information: Continued On Reverseadhi eng lrtОценок пока нет
- Reunion Questionnaire - OLDДокумент2 страницыReunion Questionnaire - OLDDiane Beaird HohenwaterОценок пока нет
- ACE Medical Center - Shareholders Personal Data Sheet-IRO HEIDIE OMBAOДокумент1 страницаACE Medical Center - Shareholders Personal Data Sheet-IRO HEIDIE OMBAOSam AlianzaОценок пока нет
- Updated-GET Global 2009 - ApplicationДокумент7 страницUpdated-GET Global 2009 - Applicationrkvance5Оценок пока нет
- FEBC Info Sheet - NEWДокумент5 страницFEBC Info Sheet - NEWnigel alinsug0% (1)
- 7-Day Divorce Without Children Worksheet PDFДокумент6 страниц7-Day Divorce Without Children Worksheet PDFmanamana95Оценок пока нет
- Velocity Health FormДокумент2 страницыVelocity Health FormChris HansenОценок пока нет
- MPDFДокумент3 страницыMPDFKbОценок пока нет
- Mnc-Cyf Member Personal Data SheetДокумент1 страницаMnc-Cyf Member Personal Data SheetMary Jane MariñoОценок пока нет
- ApplicationДокумент2 страницыApplicationGrace Deleeuw PelusoОценок пока нет
- Application For Enrollment 2010Документ2 страницыApplication For Enrollment 2010stritaschoolОценок пока нет
- Ds-260 For ClientsДокумент16 страницDs-260 For ClientsPremium77036Оценок пока нет
- Immigration Consultation Intake FormДокумент5 страницImmigration Consultation Intake FormShelby VcelkaОценок пока нет
- First Holy Communion Registration FormДокумент1 страницаFirst Holy Communion Registration FormLucy SalasОценок пока нет
- Authorization Letter TemplateДокумент1 страницаAuthorization Letter Templategarthraymundo123Оценок пока нет
- Please Complete A Form For EACH Student.: Last First Middle InitialДокумент4 страницыPlease Complete A Form For EACH Student.: Last First Middle InitialhwienОценок пока нет
- Scholarship FormДокумент3 страницыScholarship Formyaranaser246Оценок пока нет
- Bio DataДокумент2 страницыBio DataMichael Angelo BandiolaОценок пока нет
- Instructions On How To Complete A DS 160 Visa Application Big Cedar LodgeДокумент8 страницInstructions On How To Complete A DS 160 Visa Application Big Cedar LodgeGladness ChadibeОценок пока нет
- First Timers FormДокумент2 страницыFirst Timers FormLITO DELA PENAОценок пока нет
- 1 Parents Information SheetДокумент2 страницы1 Parents Information SheetVerscel Malalis GuisadioОценок пока нет
- Paper ApplicationДокумент6 страницPaper ApplicationSantosha InguvaОценок пока нет
- SCA Application Admission 2021 StudentДокумент3 страницыSCA Application Admission 2021 StudentJavan SmithОценок пока нет
- Christian Life ProgramДокумент1 страницаChristian Life ProgramGeleenОценок пока нет
- Chinese Visa Form 2023Документ3 страницыChinese Visa Form 2023Darren Kent BayocotОценок пока нет
- Community Profile FormДокумент1 страницаCommunity Profile FormEleanor GelacioОценок пока нет
- Mock College App CKДокумент14 страницMock College App CKapi-545853475Оценок пока нет
- Mentorhuntform 1Документ2 страницыMentorhuntform 1api-261719135Оценок пока нет
- Online Immigrant Visa and Alien Registration Application (DS-260)Документ11 страницOnline Immigrant Visa and Alien Registration Application (DS-260)Jordz PlaciОценок пока нет
- Teen MedicalДокумент1 страницаTeen MedicalJohn C StarkОценок пока нет
- Form of Declaration To Be Submitted by The OBC Candidate (In Addition To The Community Certificate)Документ1 страницаForm of Declaration To Be Submitted by The OBC Candidate (In Addition To The Community Certificate)RimОценок пока нет
- Missionary Application FormДокумент5 страницMissionary Application FormUOAT100% (1)
- 2017-18 YES Application-Biographical InformationДокумент1 страница2017-18 YES Application-Biographical InformationIslahОценок пока нет
- Students Personal Data With Data Privacy StatementДокумент2 страницыStudents Personal Data With Data Privacy StatementMaimaitrazoОценок пока нет
- My SocioДокумент1 страницаMy SocioLopezОценок пока нет
- North Coast Youth Ministry Application Form: General InformationДокумент4 страницыNorth Coast Youth Ministry Application Form: General InformationteejmcdeeОценок пока нет
- Online Immigrant Visa and Alien Registration Application (DS-260)Документ11 страницOnline Immigrant Visa and Alien Registration Application (DS-260)Cherrylyn Cachola100% (1)
- ZENITH INTERNATIONAL SCHOOLS Employment FormДокумент1 страницаZENITH INTERNATIONAL SCHOOLS Employment FormolootukingОценок пока нет
- ADM-FR-003 Student Directory FormДокумент2 страницыADM-FR-003 Student Directory FormRahayuОценок пока нет
- Klase Application Form.01Документ4 страницыKlase Application Form.01Kang MomenОценок пока нет
- School FormsДокумент2 страницыSchool FormslavariaserlinyОценок пока нет
- Client Interview Sheet: Jodi Head Lopez & Associates P.CДокумент7 страницClient Interview Sheet: Jodi Head Lopez & Associates P.CWilujeng HandayaniОценок пока нет
- Counseling and Testing ServicesДокумент3 страницыCounseling and Testing ServicesTuTitОценок пока нет
- Family Health History AmaДокумент5 страницFamily Health History AmaFransiscus Braveno RapaОценок пока нет
- Declearation Blank FormДокумент1 страницаDeclearation Blank Formbinodkumarnayak82Оценок пока нет
- PRC Renewal FormДокумент2 страницыPRC Renewal Formiza suarezОценок пока нет
- DateДокумент4 страницыDateapi-26391568Оценок пока нет
- Date of Marriage: - Time: - PlaceДокумент2 страницыDate of Marriage: - Time: - PlaceRosanna RebueltoОценок пока нет
- Application For Admission - Middle and High School: ApplicantДокумент2 страницыApplication For Admission - Middle and High School: ApplicantRafaelОценок пока нет
- ZuhdiJasser PDFДокумент1 страницаZuhdiJasser PDFTemple Beth SholomОценок пока нет
- Binder 1Документ5 страницBinder 1Temple Beth SholomОценок пока нет
- Oct BulletinДокумент20 страницOct BulletinTemple Beth SholomОценок пока нет
- Mishpachat Minyan 8x10Документ1 страницаMishpachat Minyan 8x10Temple Beth SholomОценок пока нет
- March of LivingДокумент1 страницаMarch of LivingTemple Beth SholomОценок пока нет
- Faith ClubДокумент1 страницаFaith ClubTemple Beth SholomОценок пока нет
- Tbs August BulletinДокумент28 страницTbs August BulletinTemple Beth SholomОценок пока нет
- WL Faith ClubДокумент1 страницаWL Faith ClubTemple Beth SholomОценок пока нет
- Religious School Calendar 2009-10Документ1 страницаReligious School Calendar 2009-10Temple Beth SholomОценок пока нет
- Application - Cover Letter 2009-2010Документ2 страницыApplication - Cover Letter 2009-2010Temple Beth SholomОценок пока нет
- Rabbi Adam Facebooknew TextДокумент1 страницаRabbi Adam Facebooknew TextTemple Beth Sholom100% (2)
- HH Guest SeatingДокумент1 страницаHH Guest SeatingTemple Beth Sholom100% (2)
- Application - Cover Letter 2009-2010Документ2 страницыApplication - Cover Letter 2009-2010Temple Beth SholomОценок пока нет
- HH Service & Programming ScheduleДокумент1 страницаHH Service & Programming ScheduleTemple Beth Sholom100% (2)
- HH Children's RegistrationДокумент1 страницаHH Children's RegistrationTemple Beth Sholom100% (2)
- Application 2009 2010Документ3 страницыApplication 2009 2010Temple Beth Sholom100% (2)
- HH Payment and Receipt SummaryДокумент1 страницаHH Payment and Receipt SummaryTemple Beth Sholom100% (2)
- HH Seating Registration FormДокумент1 страницаHH Seating Registration FormTemple Beth Sholom100% (2)
- HH Child and Teen InfoДокумент1 страницаHH Child and Teen InfoTemple Beth Sholom100% (2)
- FeeAdjustmentForm 2009Документ2 страницыFeeAdjustmentForm 2009Temple Beth SholomОценок пока нет
- New Cantor Chosen: Spring - June 2009Документ20 страницNew Cantor Chosen: Spring - June 2009Temple Beth SholomОценок пока нет
- Helping Our Kids Workshop Final PosterДокумент1 страницаHelping Our Kids Workshop Final PosterTemple Beth SholomОценок пока нет
- Cantor Dinner FlyerДокумент1 страницаCantor Dinner FlyerTemple Beth SholomОценок пока нет
- SpaDay FlyerДокумент1 страницаSpaDay FlyerTemple Beth SholomОценок пока нет
- Genetic Engineering AssignmentДокумент20 страницGenetic Engineering AssignmentAcyl Chloride HaripremОценок пока нет
- ABB FactSheet SYMS - 112018Документ2 страницыABB FactSheet SYMS - 112018Muhammad Hassan BalochОценок пока нет
- Problemas Del Capitulo 7Документ26 страницProblemas Del Capitulo 7dic vilОценок пока нет
- PIL HANDOUT in TextДокумент173 страницыPIL HANDOUT in Textbhargavi mishraОценок пока нет
- Annex B Brochure Vector and ScorpionДокумент4 страницыAnnex B Brochure Vector and ScorpionomarhanandehОценок пока нет
- Victory Magazine 2012 PDFДокумент19 страницVictory Magazine 2012 PDFijojlОценок пока нет
- Serra Do Mel 3 A 6 - Project - VC1-ReportДокумент13 страницSerra Do Mel 3 A 6 - Project - VC1-Reportjosimar gomes da silva filhoОценок пока нет
- Commercial Vehicle Aftermarket Catalog en UsДокумент56 страницCommercial Vehicle Aftermarket Catalog en UsAion RadamanthysОценок пока нет
- BA5411 ProjectGuidelines - 2020 PDFДокумент46 страницBA5411 ProjectGuidelines - 2020 PDFMonisha ReddyОценок пока нет
- PROCEMAC PT Spare Parts ManualДокумент27 страницPROCEMAC PT Spare Parts ManualMauricio CruzОценок пока нет
- E Sevai RegistrationДокумент18 страницE Sevai RegistrationSatheesh PОценок пока нет
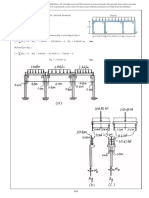
- Web Bearing and Buck1ling To BS en 1993Документ3 страницыWeb Bearing and Buck1ling To BS en 1993antoninoОценок пока нет
- IT Quiz QuestionsДокумент10 страницIT Quiz QuestionsbrittosabuОценок пока нет
- Part - A (Short Answer Questions) : S. No. Questions Bloom's Taxonomy Level Course OutcomeДокумент11 страницPart - A (Short Answer Questions) : S. No. Questions Bloom's Taxonomy Level Course OutcomeDevendra BhavsarОценок пока нет
- HP Mini 210-2120br PC Broadcom Wireless LAN Driver v.5.60.350.23 Pour Windows 7 Download GrátisДокумент5 страницHP Mini 210-2120br PC Broadcom Wireless LAN Driver v.5.60.350.23 Pour Windows 7 Download GrátisFernandoDiasОценок пока нет
- Turn Pet1 Plastic Bottles Into 3d Filament With The Recreator 3d Mk5kit Ender3 b7936987 A5e5 4b10 80fa 8754423f3ee8Документ11 страницTurn Pet1 Plastic Bottles Into 3d Filament With The Recreator 3d Mk5kit Ender3 b7936987 A5e5 4b10 80fa 8754423f3ee8Meet MehtaОценок пока нет
- Managing Apps in Windows 10Документ29 страницManaging Apps in Windows 10CourageMarumeОценок пока нет
- Arslan 20 Bba 11Документ11 страницArslan 20 Bba 11Arslan Ahmed SoomroОценок пока нет
- Nogales V Capitol Medical CenterДокумент2 страницыNogales V Capitol Medical CenterGraceОценок пока нет
- Satisfaction Attributes and Satisfaction of Customers: The Case of Korean Restaurants in BataanДокумент10 страницSatisfaction Attributes and Satisfaction of Customers: The Case of Korean Restaurants in BataanMaraОценок пока нет
- 5d814c4d6437b300fd0e227a - Scorch Product Sheet 512GB PDFДокумент1 страница5d814c4d6437b300fd0e227a - Scorch Product Sheet 512GB PDFBobby B. BrownОценок пока нет
- Tales of Mystery Imagination and Humour Edgar Allan Poe PDFДокумент289 страницTales of Mystery Imagination and Humour Edgar Allan Poe PDFmatildameisterОценок пока нет
- Mohamed Nagy Elsayed: Supply Chain ManagerДокумент6 страницMohamed Nagy Elsayed: Supply Chain Managerfasiha thathiОценок пока нет
- NV 2Документ2 страницыNV 2Joshua ApongolОценок пока нет
- 20091216-153551-APC Smart-UPS 1500VA USB SUA1500IДокумент4 страницы20091216-153551-APC Smart-UPS 1500VA USB SUA1500Ifietola1Оценок пока нет
- 5th Year PES Mrs - Hamdoud Research Methodology 2Документ3 страницы5th Year PES Mrs - Hamdoud Research Methodology 2Rami DouakОценок пока нет
- Patient Care Malaysia 2014 BrochureДокумент8 страницPatient Care Malaysia 2014 Brochureamilyn307Оценок пока нет
- LCD Television Service Manual: Chassis MTK8222 Product TypeДокумент46 страницLCD Television Service Manual: Chassis MTK8222 Product TypetvdenОценок пока нет
- Law Clinic and Mooting DR DapaahДокумент19 страницLaw Clinic and Mooting DR DapaahGlennОценок пока нет
- I. Characteristics of WastewaterДокумент59 страницI. Characteristics of WastewaterEljay VinsonОценок пока нет