Вам также может понравиться
- Skin Integrity and Wound CareДокумент38 страницSkin Integrity and Wound CareMiu MiuОценок пока нет
- Chronic Leg Edema Exercises Brochure - EN (LR) PDFДокумент2 страницыChronic Leg Edema Exercises Brochure - EN (LR) PDFsilkofosОценок пока нет
- Child Development Questionnaire 2017 v2Документ7 страницChild Development Questionnaire 2017 v2Cnellia VartolomeiОценок пока нет
- Wound Essentials 8 1 Debridement Consensus Recommendations For PracticeДокумент5 страницWound Essentials 8 1 Debridement Consensus Recommendations For PracticeAndaz MortinОценок пока нет
- Nursing Management of Pressure Ulcers in Adults PDFДокумент33 страницыNursing Management of Pressure Ulcers in Adults PDFAnindi Vivia MuktitamaОценок пока нет
- Hall Adolescent Assessment ReportДокумент3 страницыHall Adolescent Assessment Reportapi-404536886Оценок пока нет
- Anatomical TermsДокумент82 страницыAnatomical TermsRichelle Ann Gatchola EvangelistaОценок пока нет
- Australian Institute Health Welfare Aus 221Документ570 страницAustralian Institute Health Welfare Aus 221jessiebirdОценок пока нет
- Mental Capital SummaryДокумент52 страницыMental Capital SummaryaguzzzОценок пока нет
- Minor Award Name Care of The Older Person Minor Award Code 5N2706 Level 5Документ7 страницMinor Award Name Care of The Older Person Minor Award Code 5N2706 Level 5Dubes ValentinoОценок пока нет
- Updated 10-16-14 Quick Reference Guide Digital Npuap Epuap Pppia 16oct2014Документ75 страницUpdated 10-16-14 Quick Reference Guide Digital Npuap Epuap Pppia 16oct2014Anonymous kZQet6QA100% (1)
- Mental HealthДокумент146 страницMental HealthAnggraeni Beti Dwi LestariОценок пока нет
- 10 Basic First AidДокумент21 страница10 Basic First AidRUSTOM JAKEОценок пока нет
- OT 1025 - Home ModificationДокумент24 страницыOT 1025 - Home ModificationRidz FОценок пока нет
- Trauma Informed ApproachДокумент111 страницTrauma Informed Approachalejandra sarmientoОценок пока нет
- Coalition For Children Safety Around StrangersДокумент8 страницCoalition For Children Safety Around StrangersrquillinmwsuОценок пока нет
- Wound Assessment and DocumentationДокумент66 страницWound Assessment and DocumentationRiaReimannОценок пока нет
- Assessment and Mangement of Venous Leg UlcersДокумент136 страницAssessment and Mangement of Venous Leg UlcersGladys YaresОценок пока нет
- Pressure Ulcers and Hydrocolloids Made EasyДокумент6 страницPressure Ulcers and Hydrocolloids Made EasyJefferson AlexandreОценок пока нет
- BURNSДокумент16 страницBURNSRegina KadenyiОценок пока нет
- Kaleidoscope Therapy & Learning Center: Occupational Therapy Initial EvaluationДокумент7 страницKaleidoscope Therapy & Learning Center: Occupational Therapy Initial EvaluationJhudith De Julio BuhayОценок пока нет
- Basic Foot Care GuideДокумент10 страницBasic Foot Care GuidelaskarОценок пока нет
- Amputation-Dr N K BeheraДокумент8 страницAmputation-Dr N K BeheraSheel GuptaОценок пока нет
- Best Practice Recommendations For Holistic Strategies To Promote and Maintain Skin IntegrityДокумент32 страницыBest Practice Recommendations For Holistic Strategies To Promote and Maintain Skin IntegrityisaОценок пока нет
- F16 Physiotherapy After Stroke - ReferencedДокумент15 страницF16 Physiotherapy After Stroke - ReferencedMilanisti22Оценок пока нет
- Scribd PDF - Diabetic Teach PlanДокумент7 страницScribd PDF - Diabetic Teach PlanMeredith BarbОценок пока нет
- Common Diseases in ElderlyДокумент14 страницCommon Diseases in ElderlyNanang Ilham SetyajiОценок пока нет
- Defiant Children 5 Tips For DefianceДокумент7 страницDefiant Children 5 Tips For DefianceGuilleОценок пока нет
- Week 9 - Ch. 31 - SkinДокумент31 страницаWeek 9 - Ch. 31 - SkinMary SingletonОценок пока нет
- Venous Ulcer Care by Joel Arudchelvam, GC FernandoДокумент26 страницVenous Ulcer Care by Joel Arudchelvam, GC Fernandojoel arudchelvam100% (1)
- Conceptual Models of Child Malnutrition The ACF Approach in Mental Health and Care Practices 01.2013Документ76 страницConceptual Models of Child Malnutrition The ACF Approach in Mental Health and Care Practices 01.2013yayuk dwi n100% (1)
- Funda RLE RD Time TableДокумент4 страницыFunda RLE RD Time Tablemj CanilangОценок пока нет
- Addiction PDFДокумент14 страницAddiction PDFJuwita Valen RamadhanniaОценок пока нет
- SAMPLE Ergonomic Risk AssessmentДокумент6 страницSAMPLE Ergonomic Risk AssessmentRobert R. RaoОценок пока нет
- Promoting Personal Hygiene & Promoting Rest & SleepДокумент26 страницPromoting Personal Hygiene & Promoting Rest & SleepYousef JafarОценок пока нет
- Edema (Word)Документ8 страницEdema (Word)MichaelОценок пока нет
- Home Exercise ProgramДокумент6 страницHome Exercise ProgramRavin NarwalОценок пока нет
- Edema LymphedemaДокумент2 страницыEdema LymphedemaAsmat BurhanОценок пока нет
- Transferring People Safely - WebДокумент36 страницTransferring People Safely - Webkimbakicks100% (1)
- Toilet Training A Skill Development ProgrammeДокумент5 страницToilet Training A Skill Development ProgrammeKidz to Adultz ExhibitionsОценок пока нет
- Acc6075 Moving Guide TechniqueДокумент72 страницыAcc6075 Moving Guide TechniqueJasonJejametОценок пока нет
- Ebola Is Still Here: Voices From Liberia and Sierra Leone On Response and RecoveryДокумент16 страницEbola Is Still Here: Voices From Liberia and Sierra Leone On Response and RecoveryOxfamОценок пока нет
- FASD and Sexually Inappropriate Behaviors: A Guide For Criminal Justice and Forensic Mental Health ProfessionalsДокумент35 страницFASD and Sexually Inappropriate Behaviors: A Guide For Criminal Justice and Forensic Mental Health ProfessionalsfasdunitedОценок пока нет
- Iffat - Day Care Center For ElderlyДокумент11 страницIffat - Day Care Center For ElderlyRazu AhmedОценок пока нет
- New Initiatives in The Treatment of The Chronic Patient With Alcohol/substance Abuse Problems, 1987 From: TIE-Lines, Vol. 1V, No. 3, July 1987.Документ5 страницNew Initiatives in The Treatment of The Chronic Patient With Alcohol/substance Abuse Problems, 1987 From: TIE-Lines, Vol. 1V, No. 3, July 1987.Kathleen Sciacca, MA - Sciacca Comprehensive Service Dev. Dual Diagnosis; Motivational Interviewing100% (1)
- WoundsДокумент79 страницWoundsrahmanОценок пока нет
- Draping, Positioning & Pregnancy Positions: PresentsДокумент22 страницыDraping, Positioning & Pregnancy Positions: PresentsАлексОценок пока нет
- Wound CareДокумент87 страницWound CareLINDA VAN OTOOОценок пока нет
- Exercise For Older Adults FinalДокумент3 страницыExercise For Older Adults Finalapi-467445554Оценок пока нет
- Quick Reference Guide-04Dec2019Документ46 страницQuick Reference Guide-04Dec2019adiangriawanОценок пока нет
- Preterm Birth and ComplicationsДокумент5 страницPreterm Birth and Complicationsandrahlyn100% (1)
- Well Elderly InterviewДокумент2 страницыWell Elderly InterviewvalkotzenОценок пока нет
- Pruning Citrus Trees For Home LandscapesДокумент2 страницыPruning Citrus Trees For Home LandscapesRobert MorrisОценок пока нет
- Care For People With Arthritis: Evidence and Best PracticesДокумент103 страницыCare For People With Arthritis: Evidence and Best Practicespjsams119937Оценок пока нет
- Muscular System DisordersДокумент36 страницMuscular System DisordersShawn Henry CepedaОценок пока нет
- Ankle & Foot Flexibility ExercisesДокумент3 страницыAnkle & Foot Flexibility Exercisesnyeska100% (1)
- Wound ManagementДокумент86 страницWound ManagementRăzvanAndrei67% (3)
- JC - How Sleep WorksДокумент40 страницJC - How Sleep WorksLe RaОценок пока нет
- My Sexual Health Matters NSW MHCCДокумент14 страницMy Sexual Health Matters NSW MHCCRalph BrewОценок пока нет
- Manning ScoreДокумент10 страницManning ScoreYurike Natalie LengkongОценок пока нет
- The Principle of Sacramentality and Sacraments in General EditedДокумент15 страницThe Principle of Sacramentality and Sacraments in General EditedKrea QuizoОценок пока нет
- Case Study (Diabetes Mellitus)Документ24 страницыCase Study (Diabetes Mellitus)Sweetie Star88% (34)
- Basic Computations 2 IV & IVFДокумент37 страницBasic Computations 2 IV & IVFCarl Elexer Cuyugan Ano100% (5)
- Physical Assessment DocumentationДокумент12 страницPhysical Assessment DocumentationtarantineОценок пока нет
- Psychology TimelineДокумент4 страницыPsychology TimelineKrea Quizo100% (1)
- His Tory of ODДокумент13 страницHis Tory of ODAmar NathОценок пока нет
- Supplementary Notes On MT130 Module 1 and 2Документ18 страницSupplementary Notes On MT130 Module 1 and 2Junaid AkhtarОценок пока нет
- Vital Records Protection Program Guide in University of Missouri System PDFДокумент4 страницыVital Records Protection Program Guide in University of Missouri System PDFReynaldi ZulvaryanОценок пока нет
- Assessment and Treatment of Spasticity: Cori Ponter, PT, MPT, NCS Barrow Neurological Institute 3/23/19Документ76 страницAssessment and Treatment of Spasticity: Cori Ponter, PT, MPT, NCS Barrow Neurological Institute 3/23/19Praneetha100% (2)
- PD Lesson 5 Coping With Stress in Middle and Late AdolescenceДокумент16 страницPD Lesson 5 Coping With Stress in Middle and Late AdolescenceEL FuentesОценок пока нет
- Perfection: Setting StandardsДокумент2 страницыPerfection: Setting StandardsGustavo MataОценок пока нет
- Electromagnetic Interference in Critical CareДокумент4 страницыElectromagnetic Interference in Critical CareNgoc Nguyen VanОценок пока нет
- Loyola Public School, Loyola Nagar, Guntur - 522005 Promotion From Class VIII To IXДокумент1 страницаLoyola Public School, Loyola Nagar, Guntur - 522005 Promotion From Class VIII To IXDevi KalyanОценок пока нет
- BBH 411w Final Project Narrative Literature ReviewДокумент27 страницBBH 411w Final Project Narrative Literature Reviewapi-582674998Оценок пока нет
- The 12-Lead ElectrocardiogramДокумент16 страницThe 12-Lead ElectrocardiogramGrace Rivera GuarinОценок пока нет
- Página WebДокумент1 страницаPágina WebGiovanni Gil MartodimedjoОценок пока нет
- Du ProfessorsДокумент28 страницDu Professorsalka sharmaОценок пока нет
- Nursing Care - TraditionalДокумент38 страницNursing Care - Traditionalchishimba louisОценок пока нет
- Health EducationДокумент7 страницHealth Educationmylene lingonОценок пока нет
- PerDev Q3 W7-8 Detailed Lesson PlanДокумент5 страницPerDev Q3 W7-8 Detailed Lesson PlanKarieDetoreTolones100% (2)
- Competency-Based Learning Material (Common Competency)Документ45 страницCompetency-Based Learning Material (Common Competency)ZOOMTECHVOC TRAINING&ASSESSMENT100% (1)
- The Narcissist On Instagram: Epigrams and Observations - Vol IIIДокумент267 страницThe Narcissist On Instagram: Epigrams and Observations - Vol IIISam VakninОценок пока нет
- Garcia v. Salvador G.R. NO. 168512, March 20, 2007Документ9 страницGarcia v. Salvador G.R. NO. 168512, March 20, 2007ChatОценок пока нет
- DoctorsClinic Schedule March2023Документ4 страницыDoctorsClinic Schedule March2023third IIIОценок пока нет
- CO Presentation FinalДокумент56 страницCO Presentation FinalAnandОценок пока нет
- Diferencial Dislexia PDLДокумент29 страницDiferencial Dislexia PDLNádia MarquesОценок пока нет
- Paul Holmes, Steve Farnfield - The Routledge Handbook of Attachment - Implications and Interventions-Routledge (2014)Документ205 страницPaul Holmes, Steve Farnfield - The Routledge Handbook of Attachment - Implications and Interventions-Routledge (2014)Pamela Fontánez100% (4)
- A Century of Morita Therapy What Has and Has Not ChangedДокумент8 страницA Century of Morita Therapy What Has and Has Not Changedm01.abousalehОценок пока нет
- J Esthet Restor Dent - 2022 - CoachmanДокумент7 страницJ Esthet Restor Dent - 2022 - Coachmanbruno mañonОценок пока нет
- REDCOP Updates (Reg.v)Документ36 страницREDCOP Updates (Reg.v)DaNiel AUreusОценок пока нет
- Organ Transplantation Is Considered A Medical Miracle of The 20th CenturyДокумент142 страницыOrgan Transplantation Is Considered A Medical Miracle of The 20th CenturyVaibhav SharmaОценок пока нет
- COVID-19 Source Book: Third EditionДокумент64 страницыCOVID-19 Source Book: Third EditionNikolaos GonosОценок пока нет
- CPR ReportingДокумент39 страницCPR ReportingNheler SonОценок пока нет
- The Message Development Tool - A Case For Effective Operationalization of Messaging in Social Marketing PracticeДокумент17 страницThe Message Development Tool - A Case For Effective Operationalization of Messaging in Social Marketing PracticesanjayamalakasenevirathneОценок пока нет
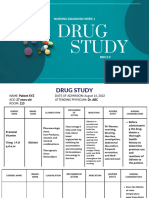
- Study: Nursing Diagnosis Week 1Документ9 страницStudy: Nursing Diagnosis Week 122 - Fernandez, Lyza Mae D.Оценок пока нет
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)От EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Рейтинг: 3 из 5 звезд3/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDОт EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDРейтинг: 5 из 5 звезд5/5 (4)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionОт EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionРейтинг: 4 из 5 звезд4/5 (404)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsОт EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsРейтинг: 4 из 5 звезд4/5 (4)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 4.5 из 5 звезд4.5/5 (82)
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (34)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryОт EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryРейтинг: 4 из 5 звезд4/5 (46)
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (6)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОт EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОценок пока нет
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeРейтинг: 2 из 5 звезд2/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsОт EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsРейтинг: 4.5 из 5 звезд4.5/5 (170)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaОт EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsОт EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsРейтинг: 5 из 5 звезд5/5 (1)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeОт EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeРейтинг: 4.5 из 5 звезд4.5/5 (2)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesОт EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesРейтинг: 4.5 из 5 звезд4.5/5 (1412)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisОт EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisРейтинг: 4.5 из 5 звезд4.5/5 (44)
- To Explain the World: The Discovery of Modern ScienceОт EverandTo Explain the World: The Discovery of Modern ScienceРейтинг: 3.5 из 5 звезд3.5/5 (51)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.От EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Рейтинг: 4.5 из 5 звезд4.5/5 (110)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsОт EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsРейтинг: 4.5 из 5 звезд4.5/5 (39)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsОт EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsОценок пока нет
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeОт EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeРейтинг: 4.5 из 5 звезд4.5/5 (254)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyОт EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyРейтинг: 4.5 из 5 звезд4.5/5 (4)