Вам также может понравиться
- Approach: A. How The Kidney Handle The Proteins?Документ9 страницApproach: A. How The Kidney Handle The Proteins?Rashed ShatnawiОценок пока нет
- Krisis HipertensiДокумент12 страницKrisis HipertensiDani NurseОценок пока нет
- Heart DiseaseДокумент38 страницHeart DiseaseDr.Sunil KumarОценок пока нет
- Idiopathic Thrombocytopenic PurpuraДокумент45 страницIdiopathic Thrombocytopenic PurpuraOhnesan Medina PerezОценок пока нет
- PericarditisДокумент29 страницPericarditisPavin KumarОценок пока нет
- Managing Psychiatric Patients in The EDДокумент28 страницManaging Psychiatric Patients in The EDfadiОценок пока нет
- Chapter 42 - Sepsis, Septic Shock, and Multiple Organ FailureДокумент15 страницChapter 42 - Sepsis, Septic Shock, and Multiple Organ FailureWorrawalun FuktongОценок пока нет
- Peripheral Artery Occlusive Disease: What To Do About Intermittent Claudication??Документ46 страницPeripheral Artery Occlusive Disease: What To Do About Intermittent Claudication??Dzariyat_Azhar_9277100% (1)
- Ely. Delirium SlidesДокумент51 страницаEly. Delirium SlidesParvathy R NairОценок пока нет
- Stem Cell TransplantationДокумент13 страницStem Cell TransplantationMylls MondejarОценок пока нет
- Lipids PowerpointДокумент15 страницLipids Powerpointapi-321789351100% (1)
- Heart Failure: An Epidemic and Public Health BurdenДокумент87 страницHeart Failure: An Epidemic and Public Health BurdenIfaОценок пока нет
- CholesterolДокумент4 страницыCholesterolapi-261438047Оценок пока нет
- PreeclampsiaДокумент34 страницыPreeclampsiaTrigo Puro100% (1)
- CardiovascularДокумент34 страницыCardiovascularRianna LarezaОценок пока нет
- Hypocalcemia, (Low Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandHypocalcemia, (Low Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Cardiac MedicationsДокумент8 страницCardiac Medicationsangeline totaram100% (2)
- Diabetes Mellitus Type 2Документ16 страницDiabetes Mellitus Type 2MTs MIFDAОценок пока нет
- Diabetic Emergencies Case StudiesДокумент32 страницыDiabetic Emergencies Case StudiesLamria Maloni Siahaan0% (1)
- Hypercalcemia, (High Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandHypercalcemia, (High Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- ECG Changes in myocardial infarctionДокумент25 страницECG Changes in myocardial infarctionginaulОценок пока нет
- Myocardialinfarction 150223043527 Conversion Gate02 PDFДокумент22 страницыMyocardialinfarction 150223043527 Conversion Gate02 PDFBhavika Aggarwal100% (1)
- Treatment of Diabetes MellitusДокумент31 страницаTreatment of Diabetes MellitusIrfan IdealistОценок пока нет
- Congestive Heart FailureДокумент19 страницCongestive Heart FailureIlavenil PanduranganОценок пока нет
- Lembar Cek LabДокумент2 страницыLembar Cek LabKarlina OktantiОценок пока нет
- LipoproteinemiaДокумент50 страницLipoproteinemiaShajeer Salim67% (6)
- Identify CVD Risk in the Office with Framingham & Non-Fasting TestsДокумент28 страницIdentify CVD Risk in the Office with Framingham & Non-Fasting TestsJuwanto Wakimin100% (1)
- Nur 111 Session 6 Sas 1Документ12 страницNur 111 Session 6 Sas 1Zzimply Tri Sha UmaliОценок пока нет
- CVDДокумент22 страницыCVDvijaymusic88100% (1)
- POLYCYTHEMIAДокумент29 страницPOLYCYTHEMIAFaizan KhanОценок пока нет
- HIV Treatment 2Документ3 страницыHIV Treatment 2kimglaidyl bontuyanОценок пока нет
- Sheehan SyndromeДокумент6 страницSheehan SyndromeArvie TagnongОценок пока нет
- Total Parenteral Nutrition Guideline-4 - 2Документ38 страницTotal Parenteral Nutrition Guideline-4 - 2Henry M. BarberenaОценок пока нет
- Von Willebrand DiseaseДокумент63 страницыVon Willebrand Diseasesaad awanОценок пока нет
- Sirs, Shock, Sepsis, ModsДокумент8 страницSirs, Shock, Sepsis, ModsthubtendrolmaОценок пока нет
- Exam 3 pathophysiology Cancer growth types and characteristicsДокумент7 страницExam 3 pathophysiology Cancer growth types and characteristicsmenickel3Оценок пока нет
- Are Viruses Living or Non-Living Organisms?Документ8 страницAre Viruses Living or Non-Living Organisms?Sydney Cloyce NagalОценок пока нет
- Rapid Response Team Whitepaper With Intro UPDATEDДокумент24 страницыRapid Response Team Whitepaper With Intro UPDATEDHari Mas KuncoroОценок пока нет
- Acute Hypertension-Hypertensive Urgency and Hypertensive EmergencyДокумент13 страницAcute Hypertension-Hypertensive Urgency and Hypertensive EmergencyAmitKumarОценок пока нет
- 6.3 Defence Against Infectious DiseaseДокумент43 страницы6.3 Defence Against Infectious DiseaseAlacrity Xenoion SpadesОценок пока нет
- Cad ....Документ94 страницыCad ....AnanthibalaОценок пока нет
- Cardiomyopathy: Imtiyaz Ali Lecturer, UTARДокумент31 страницаCardiomyopathy: Imtiyaz Ali Lecturer, UTARSalman KhanОценок пока нет
- Hyporeninemic HypoaldosteronismДокумент12 страницHyporeninemic HypoaldosteronismCésar Augusto Sánchez SolisОценок пока нет
- Thyroid Disease (Chan)Документ29 страницThyroid Disease (Chan)Sidiq AboobakerОценок пока нет
- Therapeutic Hypothermia ChillOutДокумент38 страницTherapeutic Hypothermia ChillOutJason RodmanОценок пока нет
- Vitamin B12 Deficiency and A Patient Case StudyДокумент36 страницVitamin B12 Deficiency and A Patient Case Studynherm6425100% (1)
- Immunosuppressant Drugs Drug Name Class Function Method/Receptor UseДокумент3 страницыImmunosuppressant Drugs Drug Name Class Function Method/Receptor UseKristin DouglasОценок пока нет
- Hepatitis FlashcardДокумент8 страницHepatitis Flashcardmicheal1960Оценок пока нет
- HyperglycemiaДокумент1 страницаHyperglycemiaanon_262360776Оценок пока нет
- What Is LeukemiaДокумент11 страницWhat Is LeukemiaNazneen RagasaОценок пока нет
- Normocytic Anemia'sДокумент14 страницNormocytic Anemia'sbrown_chocolate87643Оценок пока нет
- Chapter 24.child With CancerДокумент42 страницыChapter 24.child With Cancerjayme4schrankОценок пока нет
- Diabetic KetoacidosisДокумент5 страницDiabetic Ketoacidosislpickering33Оценок пока нет
- Pathogenesis of Hashimoto's Thyroiditis (Chronic Autoimmune Thyroiditis) - UpToDateДокумент22 страницыPathogenesis of Hashimoto's Thyroiditis (Chronic Autoimmune Thyroiditis) - UpToDaterazvanОценок пока нет
- Uncovering an Uncommon Cause of PsychosisДокумент2 страницыUncovering an Uncommon Cause of PsychosissavinaumarОценок пока нет
- EATING DISORDERS: Note Taking OutlineДокумент6 страницEATING DISORDERS: Note Taking OutlinePaula GarciaОценок пока нет
- Anemia: Dr. Saranya VinothДокумент45 страницAnemia: Dr. Saranya Vinothareeb khanОценок пока нет
- Reye's SyndromeДокумент11 страницReye's SyndromeChristine Go100% (1)
- Shock, Sepsis & MODSДокумент16 страницShock, Sepsis & MODSKemi Adekunle100% (1)
- Myocardial InfarctionДокумент25 страницMyocardial Infarctionfam111222Оценок пока нет
- Quiz 2 Study Guide - SHOCK!!! 25 Questions READ BOOK!!! Know Charts Esp. Stages of Shock ChartДокумент1 страницаQuiz 2 Study Guide - SHOCK!!! 25 Questions READ BOOK!!! Know Charts Esp. Stages of Shock Chartjenn1722Оценок пока нет
- ALCOHOLIC LIVER DISEASEДокумент10 страницALCOHOLIC LIVER DISEASENishanth ReddyОценок пока нет
- Calupad, Rolando Camama 1922061664Документ3 страницыCalupad, Rolando Camama 1922061664Chanel RamosОценок пока нет
- Clinical Correlation - HyperlipidemiaДокумент47 страницClinical Correlation - Hyperlipidemiamariosan81Оценок пока нет
- Cholesterol BiochemistryДокумент17 страницCholesterol BiochemistryKofi Fofie-AsieduОценок пока нет
- Quiz in Lipids (G1)Документ3 страницыQuiz in Lipids (G1)Wayne David C. PadullonОценок пока нет
- Determination of Serum LipidsДокумент2 страницыDetermination of Serum LipidsKabo Wale100% (2)
- Fatty Acid Profile of Spirulina Platensis Used AsДокумент10 страницFatty Acid Profile of Spirulina Platensis Used AsWalidur Rahman MridulОценок пока нет
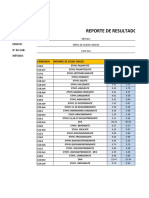
- Reporte de Resultados: Producto: Ensayo: #Ref LAB: Método: Carbonos Nombre de Ácido Graso % Área % ÁreaДокумент2 страницыReporte de Resultados: Producto: Ensayo: #Ref LAB: Método: Carbonos Nombre de Ácido Graso % Área % ÁreaHarold Isai Silvestre GómezОценок пока нет
- Average energy available from major food componentsДокумент24 страницыAverage energy available from major food componentstamani elkhairОценок пока нет
- Cell Membranes and Energy Storage: The Role of Lipids in BiologyДокумент2 страницыCell Membranes and Energy Storage: The Role of Lipids in Biologydanielle stephanieОценок пока нет
- Bridgwater Bridgwater Bridgwater Bridgwater Bridgwater, UK, Uk, Uk, Uk, UkДокумент143 страницыBridgwater Bridgwater Bridgwater Bridgwater Bridgwater, UK, Uk, Uk, Uk, Ukghee100% (1)
- New Lipid PowerpointДокумент113 страницNew Lipid PowerpointMadane Jamila Amerol SaminОценок пока нет
- Paket Pemeriksaan Kesehatan KomprehensifДокумент2 страницыPaket Pemeriksaan Kesehatan Komprehensifdedi fahrizalОценок пока нет
- LEC18 MembraneLipids 08Документ12 страницLEC18 MembraneLipids 08Mây Chính ChủОценок пока нет
- Polygenic Hypercholesterolemia: Causes, Risks & TreatmentДокумент6 страницPolygenic Hypercholesterolemia: Causes, Risks & TreatmentSamhitha Ayurvedic ChennaiОценок пока нет
- Lipoprotein Disorders 2Документ33 страницыLipoprotein Disorders 2Bolabo BenivoОценок пока нет
- Laboratory Material and Reagent Inventory ListДокумент6 страницLaboratory Material and Reagent Inventory ListWanda AguilarОценок пока нет
- Lipid ChemistryДокумент93 страницыLipid ChemistrySanreet RandhawaОценок пока нет
- Nutrition and Diet Therapy 12th Edition Roth Solutions Manual 1Документ36 страницNutrition and Diet Therapy 12th Edition Roth Solutions Manual 1richardsmithxdqnzoywcb100% (24)
- Phospholipid: From: Encyclopedia of Food Chemistry, 2019Документ8 страницPhospholipid: From: Encyclopedia of Food Chemistry, 2019Eiann Jasper LongcayanaОценок пока нет
- Protocol of Analyticon ReagentДокумент2 страницыProtocol of Analyticon ReagentmaterОценок пока нет
- LipidДокумент31 страницаLipidصالح مقالحОценок пока нет
- Test Report: Hemogram Test Name Units Results Bio. Ref. IntervalДокумент19 страницTest Report: Hemogram Test Name Units Results Bio. Ref. Intervalcs2015ok77Оценок пока нет
- Definition of LipidsДокумент18 страницDefinition of Lipidsraul sinatoОценок пока нет
- Essentiality of and Recommended Dietary Intakes For Omega-6 and Omega-3 Fatty AcidsДокумент4 страницыEssentiality of and Recommended Dietary Intakes For Omega-6 and Omega-3 Fatty AcidsRicardo CorreaОценок пока нет
- Lipid: Structure & ClassificationsДокумент25 страницLipid: Structure & ClassificationsNurul Afifah HusnaОценок пока нет
- Cholesterol SynthesisДокумент19 страницCholesterol Synthesisbrian mgabiОценок пока нет
- Bio 024 - Quiz Cfu Sas 2 (Answer Key)Документ2 страницыBio 024 - Quiz Cfu Sas 2 (Answer Key)ELLE WOODSОценок пока нет