Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- 1 s2.0 S0099239976801008 MainДокумент2 страницы1 s2.0 S0099239976801008 Main13eeeОценок пока нет
- The Precision of The Panoramic Mandibular Index: ResearchДокумент5 страницThe Precision of The Panoramic Mandibular Index: Research13eeeОценок пока нет
- Endodontic Surgery: EndodonticsДокумент28 страницEndodontic Surgery: Endodontics13eee100% (1)
- The Stressed Pulp Condition: An Endodontic-Restorative Diagnostic ConceptДокумент4 страницыThe Stressed Pulp Condition: An Endodontic-Restorative Diagnostic Concept13eeeОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Oppositional Defiant DisorderДокумент14 страницOppositional Defiant DisorderKaren ComiaОценок пока нет
- What Is Aquatic TherapyДокумент5 страницWhat Is Aquatic TherapyHaslindaОценок пока нет
- Canine Thromboembolic Disease: A Case Study and ReviewДокумент15 страницCanine Thromboembolic Disease: A Case Study and ReviewJudy ZedalisОценок пока нет
- Tes 3Документ1 страницаTes 3M Fadli FahdurohmanОценок пока нет
- Trauma Sensitive Work With Domestic Violence SurvivorsДокумент39 страницTrauma Sensitive Work With Domestic Violence SurvivorsKatrina_Woods100% (1)
- CA Treatment Phyllodes Web AlgorithmДокумент4 страницыCA Treatment Phyllodes Web AlgorithmMuhammad SubhiОценок пока нет
- Angle Class II, Division 2, Malocclusion With Deep OverbiteДокумент12 страницAngle Class II, Division 2, Malocclusion With Deep OverbiteDianaОценок пока нет
- ACLS Study GuideДокумент30 страницACLS Study GuidemmmmzОценок пока нет
- Risk Factor Stress, Depression and Suicide: Irene S. VelascoДокумент41 страницаRisk Factor Stress, Depression and Suicide: Irene S. VelascoResty FloresОценок пока нет
- Malaria ModulДокумент18 страницMalaria ModulcheiwinarnoОценок пока нет
- InjectomatTivaAgilia PDFДокумент2 страницыInjectomatTivaAgilia PDFBagas AnggerОценок пока нет
- Lyme Disease ProtocolsДокумент2 страницыLyme Disease Protocolsramaflore100% (1)
- Hyperkalemia & HypokalemiaДокумент54 страницыHyperkalemia & Hypokalemiakhangsiean89Оценок пока нет
- Psychiatry Question Bank - 65 Multiple Choice Questions On - Psychiatry in India - PDFДокумент21 страницаPsychiatry Question Bank - 65 Multiple Choice Questions On - Psychiatry in India - PDFAnkit Gupta44% (9)
- Level 1: Healing Touch Certificate ProgramДокумент2 страницыLevel 1: Healing Touch Certificate Programapi-25955699Оценок пока нет
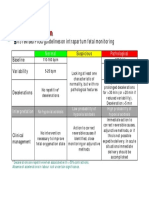
- CTG Classification PDFДокумент1 страницаCTG Classification PDFganotОценок пока нет
- How To Prevent Musculoskeletal Disorders in The WorkplaceДокумент48 страницHow To Prevent Musculoskeletal Disorders in The WorkplaceSoarin626Оценок пока нет
- Closed Fracture Neck FemurДокумент31 страницаClosed Fracture Neck FemurKiki Said100% (1)
- Play TherapyДокумент19 страницPlay TherapyKing GilgameshОценок пока нет
- Rehabilitasi Medik Pada Pasien DisfagiaДокумент21 страницаRehabilitasi Medik Pada Pasien Disfagiasevita100% (1)
- The 35 Golden Eye RulesДокумент7 страницThe 35 Golden Eye RulesTrường Giang100% (1)
- Children and Trauma A YUENДокумент16 страницChildren and Trauma A YUENMaría Soledad LatorreОценок пока нет
- Progressive Strengthening and Stretching Exercises and Ultrasound For Chronic Lateral EpicondylitisДокумент9 страницProgressive Strengthening and Stretching Exercises and Ultrasound For Chronic Lateral EpicondylitisTomBrambo100% (1)
- Motor Control ListДокумент18 страницMotor Control Listsridhar_physioОценок пока нет
- Provisional Allotment List For Third Round Ug Non-Neet Professional Courses - CompressedДокумент129 страницProvisional Allotment List For Third Round Ug Non-Neet Professional Courses - CompressedShamu AjeesОценок пока нет
- 21 Nursing ProblemДокумент32 страницы21 Nursing Problemjessell bonifacioОценок пока нет
- What Is Clinical GovernanceДокумент8 страницWhat Is Clinical GovernanceApollwn100% (1)
- Psychology - Article 38Документ1 страницаPsychology - Article 38piping stressОценок пока нет
- Manajemen Business Baby Spa Palu081119Документ19 страницManajemen Business Baby Spa Palu081119Junaedy LatolaОценок пока нет
- 16.11.24 FBonora - 15 Tips For SJT SuccessДокумент65 страниц16.11.24 FBonora - 15 Tips For SJT SuccessUmer AnwarОценок пока нет