Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Lista Carti Must HaveДокумент5 страницLista Carti Must Havediana_geambasuОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Text Original Posibil Al Sinodului, Asa Cum Apare Pe SiteДокумент19 страницText Original Posibil Al Sinodului, Asa Cum Apare Pe Sitediana_geambasuОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Marin Carciumaru Et Al., Recent Results From The Upper Palaeolithic Site of Poiana Ciresului PDFДокумент13 страницMarin Carciumaru Et Al., Recent Results From The Upper Palaeolithic Site of Poiana Ciresului PDFdiana_geambasuОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Despre Factorul IX Si CalciuДокумент5 страницDespre Factorul IX Si Calciudiana_geambasuОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Manual Hemofilie 2Документ10 страницManual Hemofilie 2diana_geambasuОценок пока нет
- ReplenineДокумент2 страницыRepleninediana_geambasuОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hemofilie January2003Документ2 страницыHemofilie January2003diana_geambasuОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- 3series Coupe CatalogueДокумент48 страниц3series Coupe Cataloguediana_geambasuОценок пока нет
- Manual Hemofilie3Документ7 страницManual Hemofilie3diana_geambasuОценок пока нет
- Samsung Galaxy s2 - User GuideДокумент164 страницыSamsung Galaxy s2 - User GuideMindfk GsОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Directive98 59 enДокумент6 страницDirective98 59 endiana_geambasuОценок пока нет
- Obiective Si Adrese Salzburg 2011-2012Документ3 страницыObiective Si Adrese Salzburg 2011-2012diana_geambasuОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- FLAVIN 7 - Study On The HematologicДокумент70 страницFLAVIN 7 - Study On The Hematologicdiana_geambasuОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- BMW Z4 CatalogueДокумент46 страницBMW Z4 Cataloguediana_geambasuОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Despre Factorul IX Si CalciuДокумент5 страницDespre Factorul IX Si Calciudiana_geambasuОценок пока нет
- Monographie FVIII ENGДокумент14 страницMonographie FVIII ENGdiana_geambasuОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- ReplenineДокумент2 страницыRepleninediana_geambasuОценок пока нет
- Manual Hemofilie4Документ2 страницыManual Hemofilie4diana_geambasuОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Manual Laborator HemofilieДокумент20 страницManual Laborator Hemofiliediana_geambasuОценок пока нет
- Lundin Etal Haemophilia 2004Документ7 страницLundin Etal Haemophilia 2004diana_geambasuОценок пока нет
- Manual Hemofilie 5Документ1 страницаManual Hemofilie 5diana_geambasuОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Manual HemofilieДокумент9 страницManual Hemofiliediana_geambasuОценок пока нет
- Manual Hemofilie 2Документ10 страницManual Hemofilie 2diana_geambasuОценок пока нет
- Delegate Registration FormДокумент2 страницыDelegate Registration Formdiana_geambasuОценок пока нет
- Despre Factorul IX Si CalciuДокумент5 страницDespre Factorul IX Si Calciudiana_geambasuОценок пока нет
- Hemofilie-Articol12 1 2005Документ10 страницHemofilie-Articol12 1 2005diana_geambasuОценок пока нет
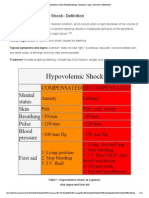
- Hypovolemic Shock Pathophysiology, Symptoms, Signs, Treatment - EHealthStarДокумент15 страницHypovolemic Shock Pathophysiology, Symptoms, Signs, Treatment - EHealthStarKaloy KamaoОценок пока нет
- Proof The Covid-19 Jabs Should Be Stopped NowДокумент2 страницыProof The Covid-19 Jabs Should Be Stopped NowDiogo MiguelОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Chapter II - Anemia and Hypovolemic Shock Secondary To An Upper Gastrointestinal BleedingДокумент3 страницыChapter II - Anemia and Hypovolemic Shock Secondary To An Upper Gastrointestinal BleedingKn VelasquezОценок пока нет
- Consent Form For Ear & Body Piercing - MCMCДокумент2 страницыConsent Form For Ear & Body Piercing - MCMCDarlОценок пока нет
- Jose Rizal Memorial State University College of Criminal Justice EducationДокумент5 страницJose Rizal Memorial State University College of Criminal Justice EducationJen PaezОценок пока нет
- McqsДокумент15 страницMcqsNazaqat FarooqОценок пока нет
- Hematology EMQДокумент7 страницHematology EMQfrabzi100% (1)
- Hemostatic AgentsДокумент18 страницHemostatic AgentshariОценок пока нет
- 443e Technique of Lumbar PunctureДокумент4 страницы443e Technique of Lumbar PunctureEXB GensanОценок пока нет
- 5 Hemodynamic Disorders, Thromboembolism and ShockДокумент162 страницы5 Hemodynamic Disorders, Thromboembolism and Shocksinte beyuОценок пока нет
- Uterine AtonyДокумент1 страницаUterine AtonyYakumaОценок пока нет
- TREMA Guidelines 1.0 EnglishДокумент22 страницыTREMA Guidelines 1.0 EnglishtremaonlineОценок пока нет
- Guidelines For The Management of Hemophilia: 2 EditionДокумент80 страницGuidelines For The Management of Hemophilia: 2 EditionMuhammad BilalОценок пока нет
- Compact: 3 EditionДокумент155 страницCompact: 3 EditionDr S n vermaОценок пока нет
- Final Patient Scenario Chapter 44 Nursing Care of Family When A Child Has A Hematologic DisorderДокумент53 страницыFinal Patient Scenario Chapter 44 Nursing Care of Family When A Child Has A Hematologic DisorderDay Meds100% (1)
- Bleeding & Coagulopathies in Clinical CareДокумент20 страницBleeding & Coagulopathies in Clinical CareKarina Mega WОценок пока нет
- Dengue 15 Minutes FlipchartДокумент18 страницDengue 15 Minutes FlipchartIsa MunsterОценок пока нет
- The 10 Commandments of Exsanguinating Pelvic Fracture ManagementДокумент14 страницThe 10 Commandments of Exsanguinating Pelvic Fracture ManagementValentin GlezОценок пока нет
- Gi BleedingДокумент22 страницыGi BleedingAndreea GociuОценок пока нет
- Thromboelastography in Cardiac SurgeryДокумент66 страницThromboelastography in Cardiac SurgeryFaisal RazaОценок пока нет
- CTC Lecture NotesДокумент28 страницCTC Lecture NotesAda WongОценок пока нет
- Herb ListДокумент42 страницыHerb ListWilliam HynesОценок пока нет
- Control Bleeding - Lesson Plan Final - C168W003 VR 1.1Документ23 страницыControl Bleeding - Lesson Plan Final - C168W003 VR 1.1RICHIEBRUSHIAОценок пока нет
- Aubrey Rose A. Vidon BSN 3Y1-2 September 4, 2020 Course Task #2Документ11 страницAubrey Rose A. Vidon BSN 3Y1-2 September 4, 2020 Course Task #2Aria0% (1)
- Periop QuizesДокумент9 страницPeriop QuizesAnonymous ZQ4gHahzОценок пока нет
- HEAD AND SPINAL INJURY - DR RetnoДокумент22 страницыHEAD AND SPINAL INJURY - DR RetnoJackОценок пока нет
- Obstetric ShockДокумент65 страницObstetric Shockkqz39931Оценок пока нет
- Dengue Update: Gan Kai XinДокумент40 страницDengue Update: Gan Kai XinKai XinОценок пока нет
- Lesson 11 CTBTДокумент2 страницыLesson 11 CTBTCookie MonsterОценок пока нет
- Hematologic DisordersДокумент197 страницHematologic DisordersDanica Mae BianitoОценок пока нет