Вам также может понравиться
- Female Reproductive System Visceral ManipuationДокумент17 страницFemale Reproductive System Visceral ManipuationFatemah Beyg100% (1)
- Myofascial Pain Syndrome in The Pelvic FloorДокумент31 страницаMyofascial Pain Syndrome in The Pelvic FlooralgomohsinОценок пока нет
- Workbook 031512 With Cover PDFДокумент197 страницWorkbook 031512 With Cover PDFIndah Yulantari100% (2)
- Effectiveness of Manual Therapy for Chronic Pelvic PainДокумент41 страницаEffectiveness of Manual Therapy for Chronic Pelvic PainMuhammadRizalN100% (1)
- Radical Unwinding Ebook PDFДокумент76 страницRadical Unwinding Ebook PDFreetiiiiОценок пока нет
- Dry Needling Courses For Pelvic Floor PhysiotherapistsДокумент9 страницDry Needling Courses For Pelvic Floor PhysiotherapistsParakram Singh Gaur0% (1)
- Cranial Rhythmic Impulse Related To The Traube-Hering-Mayer OscillationДокумент11 страницCranial Rhythmic Impulse Related To The Traube-Hering-Mayer Oscillationthe_walnutОценок пока нет
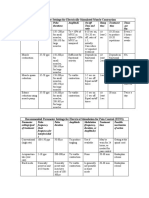
- Parameter Settings for Electrical StimulationДокумент3 страницыParameter Settings for Electrical Stimulationpallen100% (5)
- Self Myofascial ReleaseДокумент2 страницыSelf Myofascial Releasesonopuntura100% (2)
- Cervical SpineДокумент66 страницCervical SpineHotnog Madalin100% (1)
- JOHANNSON, Lisa - I Healed My Vulvodynea NaturallyДокумент44 страницыJOHANNSON, Lisa - I Healed My Vulvodynea NaturallyMariana de Oliveira100% (1)
- Chapter 7 - Management of The Hypermobile AdultДокумент19 страницChapter 7 - Management of The Hypermobile AdultDavid MansoОценок пока нет
- Trigger Point Chart Set: Torso & Extremities Paper - Anatomical Chart CompanyДокумент4 страницыTrigger Point Chart Set: Torso & Extremities Paper - Anatomical Chart Companyfesyzyzu100% (1)
- Muscle Origin Insertion Nerve Action ChartДокумент34 страницыMuscle Origin Insertion Nerve Action Chartiruizmolina100% (1)
- Compton - PsoasДокумент25 страницCompton - PsoasiruizmolinaОценок пока нет
- Pelvic Floor Physical Therapy (PDFDrive)Документ105 страницPelvic Floor Physical Therapy (PDFDrive)syed imranОценок пока нет
- Traumatic Brain Injury & Post Concussion Syndrome:Do's & Dont's A Personal Journey: TRAUMATIC BRAIN INJURY: TBI & POST-CONCUSSION SYNDOME: PCS, #2От EverandTraumatic Brain Injury & Post Concussion Syndrome:Do's & Dont's A Personal Journey: TRAUMATIC BRAIN INJURY: TBI & POST-CONCUSSION SYNDOME: PCS, #2Оценок пока нет
- Hand and Upper Extremity Review for NBCOT ExamДокумент59 страницHand and Upper Extremity Review for NBCOT ExamJenny RajanОценок пока нет
- Lumbopelvic Stability: SyllabusДокумент13 страницLumbopelvic Stability: Syllabusrapannika100% (3)
- Lymphatic Aspects of Osteopathic MedicineДокумент79 страницLymphatic Aspects of Osteopathic MedicineYuldash100% (2)
- Fascial Strain Counter Strain 2013Документ8 страницFascial Strain Counter Strain 2013Rui Pedro PereiraОценок пока нет
- Fix It With Your Hands: Reshaping Fascia for Pain Relief and Improved FunctionОт EverandFix It With Your Hands: Reshaping Fascia for Pain Relief and Improved FunctionРейтинг: 1 из 5 звезд1/5 (1)
- The Qi of Taking a Medical History and Performing a Physical ExaminationОт EverandThe Qi of Taking a Medical History and Performing a Physical ExaminationОценок пока нет
- Red Flags for Potential Serious Conditions in Patients with Pelvic, Hip, or Thigh ProblemsДокумент50 страницRed Flags for Potential Serious Conditions in Patients with Pelvic, Hip, or Thigh ProblemsAnita GajariОценок пока нет
- Swami Karmamurti Saraswati, DC, DO, Director of Satyananda Ashram, MelbourneДокумент5 страницSwami Karmamurti Saraswati, DC, DO, Director of Satyananda Ashram, MelbourneJacklynlim LkcОценок пока нет
- Myofascial Release TechniqueДокумент72 страницыMyofascial Release TechniqueAnuj Agarwal75% (4)
- The Art of Self-Adjusting: A Simple 5 Step System For Relieving Pain & TightnessОт EverandThe Art of Self-Adjusting: A Simple 5 Step System For Relieving Pain & TightnessРейтинг: 2 из 5 звезд2/5 (1)
- Unlocking Pathways of Pain: Stories of Innovative Treatments and How They WorkОт EverandUnlocking Pathways of Pain: Stories of Innovative Treatments and How They WorkОценок пока нет
- Manipulative TherapiesДокумент25 страницManipulative Therapiesapi-497063972100% (1)
- Chapman's Reflexes PointsДокумент10 страницChapman's Reflexes PointscatalinОценок пока нет
- Foot AssessmentДокумент28 страницFoot AssessmentMuskan Ahuja100% (1)
- Central SensitizationДокумент14 страницCentral SensitizationdracoscribdОценок пока нет
- 2010 The Fascial Manipulation Technique and Its Biomechanical Model: A Guide To The Human Fascial SystemДокумент3 страницы2010 The Fascial Manipulation Technique and Its Biomechanical Model: A Guide To The Human Fascial System1Rogerio100% (1)
- A Patient’s Guide to Understanding Myofascial Release: Simple Answers to Frequently Asked QuestionsОт EverandA Patient’s Guide to Understanding Myofascial Release: Simple Answers to Frequently Asked QuestionsОценок пока нет
- Counterstrain - Approaches in Osteopathic Manipulative Medicine (Friedman)Документ108 страницCounterstrain - Approaches in Osteopathic Manipulative Medicine (Friedman)Alessandro100% (2)
- Leaflet 3D Anatomy For Manual TherapiesДокумент4 страницыLeaflet 3D Anatomy For Manual Therapiestokionas100% (1)
- A Cranial Approach To Sinus Congestion: By, Nathan Widboom D.OДокумент31 страницаA Cranial Approach To Sinus Congestion: By, Nathan Widboom D.ONancyОценок пока нет
- Chapmans Reflex 457Документ8 страницChapmans Reflex 457Huram-abiОценок пока нет
- 24 Top Orthopedic TestsДокумент29 страниц24 Top Orthopedic TestsDavid Gal100% (1)
- Dermoneuromodulation treatment manualДокумент57 страницDermoneuromodulation treatment manualdasamoro100% (1)
- Relationship Between Chapman's Reflexes and Acupuncture Meridians by Traditional Chinese Medicine Practitioners in TaiwanДокумент22 страницыRelationship Between Chapman's Reflexes and Acupuncture Meridians by Traditional Chinese Medicine Practitioners in TaiwanFrederic Dubois100% (2)
- Living With PainДокумент84 страницыLiving With PainGanesh Babu100% (11)
- Holistic Healthcare For Transgender and Gender Variant Folks - Dori MidnightДокумент17 страницHolistic Healthcare For Transgender and Gender Variant Folks - Dori Midnightpille83100% (1)
- The Anatomy Trains: Connecting The Dots: Tuesday, November 20, 12Документ30 страницThe Anatomy Trains: Connecting The Dots: Tuesday, November 20, 12deemoney3Оценок пока нет
- TuxenMethod Vacuum & Decompression Therapy: Easy and Effective Soft Tissue Treatment Techniques for Professional Massage TherapistsОт EverandTuxenMethod Vacuum & Decompression Therapy: Easy and Effective Soft Tissue Treatment Techniques for Professional Massage TherapistsОценок пока нет
- A Therapist’S Guide to Understanding Myofascial Release: Simple Answers to Frequently Asked QuestionsОт EverandA Therapist’S Guide to Understanding Myofascial Release: Simple Answers to Frequently Asked QuestionsОценок пока нет
- Application of Fascial Manipulation Technique in Chronic Shoulder PainДокумент9 страницApplication of Fascial Manipulation Technique in Chronic Shoulder PainIsabelGuijarroMartinezОценок пока нет
- Motifs: The Heart of Listening Volume One by Hugh MilneДокумент1 страницаMotifs: The Heart of Listening Volume One by Hugh MilneSimon FalconiОценок пока нет
- NST Book enДокумент66 страницNST Book enMiguelGutierrez100% (2)
- Goniometry of ULДокумент55 страницGoniometry of ULshodhgangaОценок пока нет
- Terra Rosa Emag #20Документ61 страницаTerra Rosa Emag #20Terra Rosa100% (1)
- Foot and Ankle Motion PDFДокумент702 страницыFoot and Ankle Motion PDFAndrei100% (2)
- FSM Important Questions Section BДокумент1 страницаFSM Important Questions Section BRamya VasanОценок пока нет
- Aptitude 6 AnswersДокумент7 страницAptitude 6 AnswersRamya VasanОценок пока нет
- Environment Protection ActДокумент3 страницыEnvironment Protection ActRamya VasanОценок пока нет
- Asset Pricing LbsimДокумент72 страницыAsset Pricing LbsimRamya VasanОценок пока нет
- Physical Therapy Treatment of Pudendal Neuralgia: Elizabeth Rummer, MSPT Stephanie Prendergast, MPTДокумент30 страницPhysical Therapy Treatment of Pudendal Neuralgia: Elizabeth Rummer, MSPT Stephanie Prendergast, MPTRamya Vasan100% (1)
- Rubella and Congenital Rubella Syndrome in The PhilippinesДокумент9 страницRubella and Congenital Rubella Syndrome in The PhilippinesIman Ru-ancaОценок пока нет
- Chapter 20: Medicine - Set AДокумент4 страницыChapter 20: Medicine - Set ABernard Paul GuintoОценок пока нет
- Cornual Ectopic PregnancyДокумент1 страницаCornual Ectopic PregnancyPavani NallaluthanОценок пока нет
- Pill Camera PPT-1Документ19 страницPill Camera PPT-1Sara VijayОценок пока нет
- Update GINA 2006Документ29 страницUpdate GINA 2006Anka EremiaОценок пока нет
- Little Harwood Health Centre Practice LeafletДокумент5 страницLittle Harwood Health Centre Practice Leafletkovi mОценок пока нет
- Cardiac Pharmacology Questions for Evolve ExamДокумент5 страницCardiac Pharmacology Questions for Evolve ExamAmanda SimpsonОценок пока нет
- Electronic News Letter From Travancore Medical CollegeДокумент4 страницыElectronic News Letter From Travancore Medical Collegetummalapalli venkateswara raoОценок пока нет
- Tracing Chronic Fatigue Syndrome Tsfunction Is Key To ME - CFS - B Day PDFДокумент91 страницаTracing Chronic Fatigue Syndrome Tsfunction Is Key To ME - CFS - B Day PDFsanthigiОценок пока нет
- Hospital Information SystemДокумент2 страницыHospital Information SystemManpreetaaОценок пока нет
- Nurs 603 Assignment 1 Objective Tests Design and Considerations Final For SubmissionДокумент13 страницNurs 603 Assignment 1 Objective Tests Design and Considerations Final For Submissionapi-323169345Оценок пока нет
- Bipolar Disorder ProjectДокумент5 страницBipolar Disorder ProjectRitika100% (2)
- Yalom Momma and The Meaning of LifeДокумент15 страницYalom Momma and The Meaning of LifeKatya Black0% (1)
- Dengue Is Transmitted by The Bite of An Aedesmosquito Infected With Any One of The Four DengueДокумент6 страницDengue Is Transmitted by The Bite of An Aedesmosquito Infected With Any One of The Four DengueKatrina PonceОценок пока нет
- LTCW Breast Write UpДокумент21 страницаLTCW Breast Write Upapi-632682404Оценок пока нет
- Teaching Project - BPДокумент22 страницыTeaching Project - BPapi-283482759Оценок пока нет
- ABДокумент44 страницыAByustinaОценок пока нет
- Retroperitoneal LymphangiomaДокумент78 страницRetroperitoneal LymphangiomaAnishChowdhuryОценок пока нет
- Case Study On PROMДокумент11 страницCase Study On PROMPabhat Kumar86% (7)
- PlabДокумент28 страницPlabK Vijay KumarОценок пока нет
- How gastric acid aids digestion and the pathophysiology of peptic ulcersДокумент4 страницыHow gastric acid aids digestion and the pathophysiology of peptic ulcersh00rpariОценок пока нет
- Imaging Features of Sarcoidosis On MDCT, FDG PET, and PET/CTДокумент6 страницImaging Features of Sarcoidosis On MDCT, FDG PET, and PET/CTALE X RAYОценок пока нет
- Cipp 2015 AbstractsДокумент88 страницCipp 2015 AbstractsBuyanaaRise100% (2)
- Precision Attachments For The 21st CenturyДокумент6 страницPrecision Attachments For The 21st CenturyMohsin Habib67% (3)
- Dorothea Orem TheoryДокумент40 страницDorothea Orem TheoryIndra Doank100% (2)
- CPC Sample Questions 2020Документ6 страницCPC Sample Questions 2020manju80% (5)
- HyperthermiaДокумент40 страницHyperthermiaqaisersiddi100% (2)
- (212006973) 49692851-NCP-Sleep-DeprivationДокумент3 страницы(212006973) 49692851-NCP-Sleep-DeprivationIsabel Barredo Del MundoОценок пока нет
- Inner Demon Destroyer MakeshiftДокумент18 страницInner Demon Destroyer MakeshiftMike H100% (1)
- What Is Hashimoto's Disease?Документ6 страницWhat Is Hashimoto's Disease?Novia MentariОценок пока нет