Вам также может понравиться
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Common Cardiac MedicationsДокумент1 страницаCommon Cardiac MedicationsPaige HardekopfОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Blood Collection TubesДокумент4 страницыBlood Collection TubesJilajeet Goswami100% (2)
- 13 Areas of Assessment (Tomas Claudio Memorial College)Документ14 страниц13 Areas of Assessment (Tomas Claudio Memorial College)jorden36067% (3)
- Introduction To BioethicsДокумент15 страницIntroduction To BioethicsMaureen A. Bawang100% (3)
- Analysis of The Socket Bone Wall Dimensions in The Upper Maxilla in Relation To Immediate Implant PlacementДокумент6 страницAnalysis of The Socket Bone Wall Dimensions in The Upper Maxilla in Relation To Immediate Implant PlacementLeonardo PolitoОценок пока нет
- How To Conduct A Mock TracerДокумент10 страницHow To Conduct A Mock Tracerngurah_wardana100% (1)
- En - 2025-123-1837662383-Nursing KPI 2013 - FINALДокумент9 страницEn - 2025-123-1837662383-Nursing KPI 2013 - FINALIamnurse NylejОценок пока нет
- KATH - DCH Treatment GuidelinesДокумент173 страницыKATH - DCH Treatment GuidelinesCarterine ListОценок пока нет
- Sensory DeprivationДокумент29 страницSensory Deprivationsangeetha francis100% (1)
- Inference Based Therapy Fo BDD PDFДокумент10 страницInference Based Therapy Fo BDD PDFGeniefe VivendaОценок пока нет
- DOH AO 2016-0041 Prevention and Management of Abortion ComplicationsДокумент13 страницDOH AO 2016-0041 Prevention and Management of Abortion ComplicationsGa B B Orlongan100% (1)
- CRM Practices in Hospitals: (Case of Fortis Hospital)Документ14 страницCRM Practices in Hospitals: (Case of Fortis Hospital)Dinesh Shende89% (9)
- "Psychology Works" Fact Sheet:: Obsessive Compulsive DisorderДокумент4 страницы"Psychology Works" Fact Sheet:: Obsessive Compulsive DisorderDedy HariwijayaОценок пока нет
- Hospital PlanningДокумент24 страницыHospital PlanningDees_24Оценок пока нет
- Side Effects of NSAIDsДокумент8 страницSide Effects of NSAIDsAlmas PrawotoОценок пока нет
- Austin Journal of Tropical Medicine & HygieneДокумент5 страницAustin Journal of Tropical Medicine & HygieneAustin Publishing GroupОценок пока нет
- Professionals and Practitioners in CounselingДокумент20 страницProfessionals and Practitioners in CounselingJac KieОценок пока нет
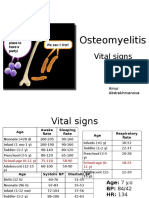
- PBL 2 - OsteomyelitisДокумент10 страницPBL 2 - OsteomyelitisAinur AbdrakhmanovaОценок пока нет
- RNTCPДокумент30 страницRNTCPDeepa SharmaОценок пока нет
- Case Study of A Boy With HaemophiliaДокумент18 страницCase Study of A Boy With HaemophiliaImanuel Far-FarОценок пока нет
- 405 Genetics of DementiaДокумент12 страниц405 Genetics of DementiaLulu LuwiiОценок пока нет
- Hematology - Oncology GlossaryДокумент18 страницHematology - Oncology GlossaryFran CescaОценок пока нет
- Ivp Dari WikipediaДокумент6 страницIvp Dari Wikipediabellatrix orionОценок пока нет
- PromixineДокумент2 страницыPromixineStelaA1Оценок пока нет
- NURSES FDARE PROGRESS NOTES REVISED SampleДокумент2 страницыNURSES FDARE PROGRESS NOTES REVISED Samplehannahmagdadaro0402Оценок пока нет
- A Comparative Study of Intrathecal Injection of Bupivacaine Alone or With Fentanyl, Clonidine, and Neostigmine in Lower Abdominal SurgeriesДокумент16 страницA Comparative Study of Intrathecal Injection of Bupivacaine Alone or With Fentanyl, Clonidine, and Neostigmine in Lower Abdominal SurgeriesdhiyaОценок пока нет
- Medical Emergency Teams/Rapid Response Teams: Purpose and BenefitsДокумент2 страницыMedical Emergency Teams/Rapid Response Teams: Purpose and BenefitsPsc CilegonОценок пока нет
- Ebp Presentation 1Документ21 страницаEbp Presentation 1api-340248301Оценок пока нет
- Jurnal Biokimia KalsiumДокумент5 страницJurnal Biokimia KalsiumdimitriprawiraОценок пока нет
- Auriculotherapy For Pain Management: A Systematic Review and Meta-Analysis of Randomized Controlled TrialsДокумент12 страницAuriculotherapy For Pain Management: A Systematic Review and Meta-Analysis of Randomized Controlled TrialsSol Instituto TerapêuticoОценок пока нет