Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Roadmap: B1+ Students' Book Audio ScriptsДокумент44 страницыRoadmap: B1+ Students' Book Audio ScriptsThanh Dat Phan100% (4)
- BF02692337 PDFДокумент2 страницыBF02692337 PDFHitesh LokeОценок пока нет
- MSDS Aradur 2965 PDFДокумент9 страницMSDS Aradur 2965 PDFkamalnandreОценок пока нет
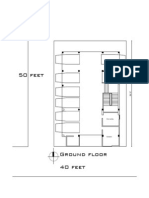
- Ground FloorДокумент1 страницаGround FloorAnimesh23Оценок пока нет
- Ground Floor Presentation Plan: Stair Toilet 6'-1"X3'-11" Toilet 5'-8"X3'-11" Parking ParkingДокумент1 страницаGround Floor Presentation Plan: Stair Toilet 6'-1"X3'-11" Toilet 5'-8"X3'-11" Parking ParkingAnimesh23Оценок пока нет
- Lift (01) Lift (02) : Detail of Ground Floor Lift Lobby & Reception DetailДокумент1 страницаLift (01) Lift (02) : Detail of Ground Floor Lift Lobby & Reception DetailAnimesh23Оценок пока нет
- The Requirements: Means of VentilationДокумент6 страницThe Requirements: Means of VentilationAnimesh23Оценок пока нет
- The Requirements: Means of VentilationДокумент6 страницThe Requirements: Means of VentilationAnimesh23Оценок пока нет
- Ad-Din Children's Hospital, JessoreДокумент4 страницыAd-Din Children's Hospital, JessoreAnimesh23Оценок пока нет
- Server Room GuidelinesДокумент2 страницыServer Room GuidelinesAnimesh23100% (1)
- Catálogo DP InglêsДокумент20 страницCatálogo DP Inglêsjf2003Оценок пока нет
- E2870-13 Standard Test Method For Evaluating RelativДокумент6 страницE2870-13 Standard Test Method For Evaluating RelativA MusaverОценок пока нет
- Favino Circulation of Scientific Knowledge AcroДокумент8 страницFavino Circulation of Scientific Knowledge AcroPeter FryОценок пока нет
- Air Tunnels: Submitted By: Priyanka Sinha SK MD Sibli Akram Ananya Sreyansri NandaДокумент8 страницAir Tunnels: Submitted By: Priyanka Sinha SK MD Sibli Akram Ananya Sreyansri NandaPriyanka SinhaОценок пока нет
- Version 2 Dog Legged Stair ES EN 1992-1-1 2015Документ29 страницVersion 2 Dog Legged Stair ES EN 1992-1-1 2015Khaja100% (2)
- Sawla - Laska (Lot - I) Road Project Hydrology - Hydraulics MДокумент64 страницыSawla - Laska (Lot - I) Road Project Hydrology - Hydraulics Mashe zinab100% (2)
- Growth Rate and Fattening Potetial of Meat AnimalsДокумент54 страницыGrowth Rate and Fattening Potetial of Meat AnimalsMuhammad Shahzad ChandiaОценок пока нет
- Anritsu Metal Detection GuideДокумент32 страницыAnritsu Metal Detection GuideJesus Roberto De La Vega GermanОценок пока нет
- ABB Photovoltaic DisconnectorsДокумент6 страницABB Photovoltaic DisconnectorsBog PenОценок пока нет
- Furuno FM 8700 Users Manual 429122Документ102 страницыFuruno FM 8700 Users Manual 429122Igor MaranguanheОценок пока нет
- Paracetamol BPДокумент4 страницыParacetamol BPjaimurugeshОценок пока нет
- Portland PortДокумент18 страницPortland PortAnonymous Lx3jPjHAVLОценок пока нет
- 1-Theory of Metal Cutting PDFДокумент144 страницы1-Theory of Metal Cutting PDFNithinArvindОценок пока нет
- Harrington SOAP NoteДокумент5 страницHarrington SOAP NoteDanielle100% (4)
- 7UM512 CatalogueДокумент12 страниц7UM512 Cataloguebuianhtuan1980Оценок пока нет
- YearbookДокумент55 страницYearbookGODWIN IRIMORENОценок пока нет
- ISNGI 2017 ProgrammeДокумент6 страницISNGI 2017 ProgrammeJoanna JohnsonОценок пока нет
- Devi Narayaneeyam - Dasakam 9 Bhuvaneswari Darsanam - Seeing of BhuvaneswariДокумент7 страницDevi Narayaneeyam - Dasakam 9 Bhuvaneswari Darsanam - Seeing of BhuvaneswaribrindaОценок пока нет
- Benzene and Phenol (25-05-2023)Документ55 страницBenzene and Phenol (25-05-2023)hibajama72Оценок пока нет
- Rate List of 1-June-2015 To 31-May-2016: S.No Code Test Name Standard Rates 15% Discounted RatesДокумент25 страницRate List of 1-June-2015 To 31-May-2016: S.No Code Test Name Standard Rates 15% Discounted RatesMirza BabarОценок пока нет
- CON21 6th EditionДокумент65 страницCON21 6th EditionDavid WeeОценок пока нет
- IoT & WSN - Module 5 - 2018 by Prof - SVДокумент43 страницыIoT & WSN - Module 5 - 2018 by Prof - SVVignesh MJ83% (6)
- Aqa Econ3 QP Jan12Документ8 страницAqa Econ3 QP Jan12api-247036342Оценок пока нет
- GPT Protocol - Trypcase Soy AgarДокумент8 страницGPT Protocol - Trypcase Soy AgarmailboxofmurliОценок пока нет
- Feu Sharing Stress MNGTДокумент58 страницFeu Sharing Stress MNGTsquidsexoОценок пока нет
- Kasuti of KarnatakaДокумент2 страницыKasuti of KarnatakarhlkОценок пока нет
- Run Omega Run Lunar Omegaverse Book 5 Shyla Colt All ChapterДокумент52 страницыRun Omega Run Lunar Omegaverse Book 5 Shyla Colt All Chapterkate.brown975100% (6)