Вам также может понравиться
- 2011 Sex Workers Gap Analysis ReportДокумент68 страниц2011 Sex Workers Gap Analysis ReportOfficeОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Pelvic Inflammatory DiseaseДокумент3 страницыPelvic Inflammatory DiseaseRania S. HamdanОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- PD Gyne ReviewerДокумент2 страницыPD Gyne ReviewerKristine Boholst100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Human Sexuallity Midterm ReviewДокумент15 страницHuman Sexuallity Midterm ReviewugomiesterОценок пока нет
- EpididymitisДокумент8 страницEpididymitisShafira WidiaОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- DR Neeta Warty ProfileДокумент10 страницDR Neeta Warty Profilecount.bluesОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Pelvic Inflammatory DiseaseДокумент8 страницPelvic Inflammatory DiseaseAndyan Adlu Prasetyaji0% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- B) Reassurance That This Is Normal InitiallyДокумент51 страницаB) Reassurance That This Is Normal InitiallygofisheeОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- 12 Best IVF Doctors in Bangalore With High Success RatesДокумент8 страниц12 Best IVF Doctors in Bangalore With High Success RatesPrabha SharmaОценок пока нет
- Karim NagarДокумент8 страницKarim NagarAbhinavReddyОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- NCM 109 Midterms - Infertility L2Документ7 страницNCM 109 Midterms - Infertility L2Leigh Angelika Dela CruzОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- (Ebook) Sex Guide - Special Cunnilingus Techniques and SecretsДокумент5 страниц(Ebook) Sex Guide - Special Cunnilingus Techniques and Secretsbonnie_caseyОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
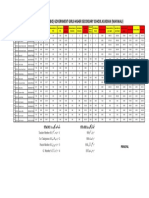
- Merit List Stis (Bio) Government Girls Higher Secondary School Kundian (Mianwali)Документ1 страницаMerit List Stis (Bio) Government Girls Higher Secondary School Kundian (Mianwali)Malik AsadОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Legalization of Abortion in The PhilippinesДокумент2 страницыLegalization of Abortion in The PhilippinesMary Kaye SilvestreОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Ten-Step Vaginal Hysterectomy - A Newer and Better ApproachДокумент8 страницThe Ten-Step Vaginal Hysterectomy - A Newer and Better ApproachqisthiaufaОценок пока нет
- CelibacyДокумент3 страницыCelibacyHoney De LeonОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- SBA Handbook For SN ANM PDFДокумент69 страницSBA Handbook For SN ANM PDFKripa Susan100% (2)
- Men and Chlamydia ScreeningДокумент28 страницMen and Chlamydia ScreeningMen's Health ForumОценок пока нет
- Chapter IДокумент7 страницChapter IRenze Meinard MortigaОценок пока нет
- A American Sex SurveyДокумент27 страницA American Sex SurveyRamesh RajagopalanОценок пока нет
- Sexually Transmitted DiseasesДокумент76 страницSexually Transmitted Diseasessomaya abdulhakimОценок пока нет
- Republic of The Philippines Department of Education Region I Division of La Union San Juan District Second Quarter Name: - ScoreДокумент3 страницыRepublic of The Philippines Department of Education Region I Division of La Union San Juan District Second Quarter Name: - ScoreMary Jane Acierto-cuello100% (3)
- Raveno Amaral - 1111013058 - OvidrelДокумент19 страницRaveno Amaral - 1111013058 - OvidrelIka RizkyОценок пока нет
- AidsДокумент3 страницыAidsmehulj099Оценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Position PaperДокумент2 страницыPosition Paperangelo pamatianОценок пока нет
- Contraception MethodsДокумент38 страницContraception MethodsDaisy NdhlovuОценок пока нет
- Sexually Transmitted Diseases: Summary of CDC Treatment GuidelinesДокумент3 страницыSexually Transmitted Diseases: Summary of CDC Treatment GuidelinesSumate KittiОценок пока нет
- What Is Microsurgical Tubal Ligation Reversal?Документ2 страницыWhat Is Microsurgical Tubal Ligation Reversal?Andy WijayaОценок пока нет
- Case Presentation Dr. Rutmila Rahman11.12.22Документ15 страницCase Presentation Dr. Rutmila Rahman11.12.22Spinothalamic tractОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Condom Use and Associated Factors Among Hiv PDFДокумент114 страницCondom Use and Associated Factors Among Hiv PDFBuleloОценок пока нет