Вам также может понравиться
- In Total With Result 1Документ65 страницIn Total With Result 1arshad khanОценок пока нет
- OM AssignmentДокумент18 страницOM AssignmentYoosuf Mohamed IrsathОценок пока нет
- A Study of Patient Satisfaction Level in Out Patient Department (OPD) in A Tertiary Care Hospital in MaharashtraДокумент9 страницA Study of Patient Satisfaction Level in Out Patient Department (OPD) in A Tertiary Care Hospital in MaharashtraVital TejaОценок пока нет
- Running Head: Patient-Centered Care 1Документ9 страницRunning Head: Patient-Centered Care 1Anonymous mZC2qZОценок пока нет
- Dimensions of Patient Experience in Addiction and Mental HealthДокумент11 страницDimensions of Patient Experience in Addiction and Mental HealthVĩ Vũ NgọcОценок пока нет
- The Impact of The Payment of The Nursing Fee On The Quality of Clinical Services and The Satisfaction of Service RecipientsДокумент18 страницThe Impact of The Payment of The Nursing Fee On The Quality of Clinical Services and The Satisfaction of Service Recipientsindex PubОценок пока нет
- Value in Health CareДокумент6 страницValue in Health CareLady ZahraОценок пока нет
- Patient Empowerment BMC Health Services Research2012Документ8 страницPatient Empowerment BMC Health Services Research2012Constantino SantosОценок пока нет
- Patient Centredness and QualityДокумент7 страницPatient Centredness and QualityAntonelle BeharryОценок пока нет
- NHS contributions to quality healthcare and social careДокумент15 страницNHS contributions to quality healthcare and social careYogita BhandariОценок пока нет
- Patients Satisfaction: To Analyse The Patients Satisfaction Towards The Treatment by The HospitalДокумент4 страницыPatients Satisfaction: To Analyse The Patients Satisfaction Towards The Treatment by The HospitalGen EswarОценок пока нет
- Understanding Patients' Perception and Experience in Improving Quality Healthcare With One of The Leading Public Hospitals in ErbilДокумент26 страницUnderstanding Patients' Perception and Experience in Improving Quality Healthcare With One of The Leading Public Hospitals in ErbilKemal Surji PhD RRTОценок пока нет
- Asamrew (2020) Level of Patient Satisfaction With Inpatient Services and Its Determinants A Study of A Specialized Hospital in EthiopiaДокумент12 страницAsamrew (2020) Level of Patient Satisfaction With Inpatient Services and Its Determinants A Study of A Specialized Hospital in EthiopiaDiego RiveraОценок пока нет
- Registration 1Документ4 страницыRegistration 1Gupta PrkОценок пока нет
- Session 12 - Performance Outcomes in HealthCareДокумент15 страницSession 12 - Performance Outcomes in HealthCarefreshglow.lkОценок пока нет
- Licensure, Accreditation, and CertificationДокумент62 страницыLicensure, Accreditation, and CertificationSohib KawaiОценок пока нет
- Patient-Centered Care in Nursing and DentistryДокумент15 страницPatient-Centered Care in Nursing and DentistryJan Karl PreciosoОценок пока нет
- PNACF510Документ56 страницPNACF510Jerusalem ShiferawОценок пока нет
- Assessing Healthcare QualityДокумент30 страницAssessing Healthcare QualityAnonymous TO9fMjОценок пока нет
- Pengalaman Pasien ExeДокумент17 страницPengalaman Pasien ExesoniОценок пока нет
- An Information Revolution and Greater Choice and Control Webchat: Follow Up QuestionsДокумент21 страницаAn Information Revolution and Greater Choice and Control Webchat: Follow Up QuestionsDepartmentofHealthОценок пока нет
- Chapter # 01Документ49 страницChapter # 01md.jewel ranaОценок пока нет
- CMA PuttДокумент16 страницCMA PuttShafffОценок пока нет
- 2020 Model and Process For Nutrition and Dietetic Practice 1Документ20 страниц2020 Model and Process For Nutrition and Dietetic Practice 1Saba TanveerОценок пока нет
- Measuring Patient Satisfaction in HealthcareДокумент71 страницаMeasuring Patient Satisfaction in HealthcareAncy Sunny100% (1)
- Aims & ObjectivesДокумент9 страницAims & ObjectivesChandranath ChakrabortyОценок пока нет
- AHA Patient Centered Medical HomeДокумент21 страницаAHA Patient Centered Medical Homein678Оценок пока нет
- A Purchaser's Guide To Understanding Thethe Medical Home ModelДокумент40 страницA Purchaser's Guide To Understanding Thethe Medical Home ModelPatient-Centered Primary Care CollaborativeОценок пока нет
- Consumer Perception On Service Quality in Health Care SectorДокумент4 страницыConsumer Perception On Service Quality in Health Care SectorAmit Chauhan R.Оценок пока нет
- Getting StartedДокумент22 страницыGetting StartedOSCAR CONTRERASОценок пока нет
- GettingStarted AmbulatoryCareДокумент35 страницGettingStarted AmbulatoryCareSreya SanilОценок пока нет
- Chapter 1Документ41 страницаChapter 1HazelОценок пока нет
- cf_summary_report_template (1).edited (1)Документ4 страницыcf_summary_report_template (1).edited (1)EVAN KIPKEMOIОценок пока нет
- Value Based HealthcareДокумент48 страницValue Based HealthcareAsem Shadid100% (1)
- Turning The Vision of Connected Health Into A RealityДокумент14 страницTurning The Vision of Connected Health Into A RealityCognizant100% (2)
- 2 Zibemr Vol1 Issue3Документ11 страниц2 Zibemr Vol1 Issue3Yulinur FirdausОценок пока нет
- In Patient Satisfaction Survey-How Does It Help Our Health Care Delivery System (The Patient, The Health Care Giver and The Organization) ?Документ10 страницIn Patient Satisfaction Survey-How Does It Help Our Health Care Delivery System (The Patient, The Health Care Giver and The Organization) ?Pallavi PalluОценок пока нет
- QultypaperwithAaron PDFДокумент12 страницQultypaperwithAaron PDFumie khoirunОценок пока нет
- Aspects of Quality Management PlanДокумент16 страницAspects of Quality Management PlanJohnОценок пока нет
- CP Alliance 10 Measure CriteriaДокумент11 страницCP Alliance 10 Measure Criteriaiggybau100% (1)
- Regional Health Improvement Collaboratives: Overcoming Barriers to Healthcare ReformДокумент25 страницRegional Health Improvement Collaboratives: Overcoming Barriers to Healthcare ReformTimothy Suraj0% (1)
- Final Paper Satisfaction 2015Документ18 страницFinal Paper Satisfaction 2015Ananga ChakrabortyОценок пока нет
- Collaborative CareДокумент16 страницCollaborative CareArdhani IrfanОценок пока нет
- Qms Project #1Документ16 страницQms Project #1GirumОценок пока нет
- Developing A Total Quality Management Framework For Healthcare OrganizationsДокумент10 страницDeveloping A Total Quality Management Framework For Healthcare Organizationsmahadabrata21Оценок пока нет
- Quality Improvement Made SimpleДокумент67 страницQuality Improvement Made Simpledan iacobОценок пока нет
- Georgiana Icon College - Operations Management (MIHAELA PALAGA OMQE 1)Документ17 страницGeorgiana Icon College - Operations Management (MIHAELA PALAGA OMQE 1)Swapneel DeyОценок пока нет
- Patient Satisfaction SurveyДокумент113 страницPatient Satisfaction SurveyCherry Mae L. Villanueva100% (1)
- Family Medicine Clerkship QI and Population Health ToolkitДокумент36 страницFamily Medicine Clerkship QI and Population Health ToolkitjhhjjhОценок пока нет
- Group 9 Planing Dental ServicesДокумент26 страницGroup 9 Planing Dental ServicesMAYORMITA SHEBERLYN KYEОценок пока нет
- Singh 2017Документ8 страницSingh 2017lulukzОценок пока нет
- Framework On Integrated People-Centred Health Services (IPCHS)Документ23 страницыFramework On Integrated People-Centred Health Services (IPCHS)Merty ReferendumОценок пока нет
- Factors Influencing Customer Satisfaction in Healthcare ServicesДокумент152 страницыFactors Influencing Customer Satisfaction in Healthcare Servicesumar100% (5)
- Leadership for Interprofessional CollaborationДокумент16 страницLeadership for Interprofessional CollaborationKimberly AvendanoОценок пока нет
- Physiotherapy - Vol 94 - N2 2008Документ86 страницPhysiotherapy - Vol 94 - N2 2008sputnickОценок пока нет
- Clinical Governance in The UK NHSДокумент4 страницыClinical Governance in The UK NHSchiefsanjivОценок пока нет
- Textbook of Urgent Care Management: Chapter 41, Measuring and Improving Patient SatisfactionОт EverandTextbook of Urgent Care Management: Chapter 41, Measuring and Improving Patient SatisfactionОценок пока нет
- Therapy Outcome Measures for Rehabilitation Professionals: Speech and Language Therapy, Physiotherapy, Occupational TherapyОт EverandTherapy Outcome Measures for Rehabilitation Professionals: Speech and Language Therapy, Physiotherapy, Occupational TherapyОценок пока нет
- Using ISO 9001 in Healthcare: Applications for Quality Systems, Performance Improvement, Clinical Integration, and AccreditationОт EverandUsing ISO 9001 in Healthcare: Applications for Quality Systems, Performance Improvement, Clinical Integration, and AccreditationОценок пока нет
- AnestesiiДокумент1 страницаAnestesiiCyntia Agus AcehОценок пока нет
- Pasword Enjoy CafeДокумент1 страницаPasword Enjoy CafeCyntia Agus AcehОценок пока нет
- Recent Manag Ement of Hypertencive EmergenciesДокумент32 страницыRecent Manag Ement of Hypertencive EmergenciesCyntia Agus AcehОценок пока нет
- Shock Syndrome-2005Документ62 страницыShock Syndrome-2005Cyntia Agus AcehОценок пока нет
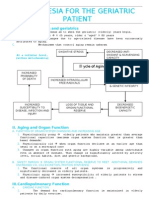
- 6.anesthesia For The Geriatric PatientДокумент5 страниц6.anesthesia For The Geriatric PatientCyntia Agus AcehОценок пока нет
- The Golden Hour: Is The Time in Which Resuscitation of Severely Injured Patients Must Begin To Achieve Maximal SurviveДокумент17 страницThe Golden Hour: Is The Time in Which Resuscitation of Severely Injured Patients Must Begin To Achieve Maximal SurviveCyntia Agus AcehОценок пока нет
- Nutrisi Enteral - LectureДокумент26 страницNutrisi Enteral - LectureNicholas PetrovskiОценок пока нет
- Shock Syndrome-2005Документ62 страницыShock Syndrome-2005Cyntia Agus AcehОценок пока нет
- Oxygen TherapyДокумент24 страницыOxygen TherapyCyntia Agus AcehОценок пока нет
- ECG, Block Intraventricular, Preexcitation (Rev)Документ25 страницECG, Block Intraventricular, Preexcitation (Rev)Cyntia Agus AcehОценок пока нет
- CheatДокумент2 страницыCheatsdnpaketiban02Оценок пока нет
- F-16 Multirole Fighter Cheats and TipsДокумент1 страницаF-16 Multirole Fighter Cheats and TipsCyntia Agus AcehОценок пока нет
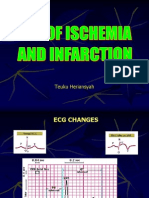
- ECG, Ischemia, MCI (Rev)Документ28 страницECG, Ischemia, MCI (Rev)Cyntia Agus AcehОценок пока нет
- Pasword Enjoy CafeДокумент1 страницаPasword Enjoy CafeCyntia Agus AcehОценок пока нет
- Installation ReadmeДокумент11 страницInstallation ReadmeCyntia Agus AcehОценок пока нет
- A Cute Appendic ItsДокумент109 страницA Cute Appendic ItsYosevine Noviana PeranginanginОценок пока нет
- Pasword Enjoy CafeДокумент1 страницаPasword Enjoy CafeCyntia Agus AcehОценок пока нет