Вам также может понравиться
- Algorithms To Guide Your Diagnosis & TreatmentДокумент244 страницыAlgorithms To Guide Your Diagnosis & TreatmentHasan Pallab MarufОценок пока нет
- Caplan, Michael J-Reference Module in Biomedical Research-Elsevier (2014) PDFДокумент17 страницCaplan, Michael J-Reference Module in Biomedical Research-Elsevier (2014) PDFMuhammad IkbarОценок пока нет
- Valvular Heart DiseaseДокумент27 страницValvular Heart DiseaseOwen J. WieseОценок пока нет
- Pathophysiology of Cardiogenic Pulmonary EdemaДокумент8 страницPathophysiology of Cardiogenic Pulmonary EdemaLili Fiorela CRОценок пока нет
- Anemia PDFДокумент11 страницAnemia PDFRegieLimos100% (1)
- Elitox PPT ENG CompressedДокумент18 страницElitox PPT ENG CompressedTom ArdiОценок пока нет
- Shock and Circulatory FailureДокумент8 страницShock and Circulatory FailureOktaviana Sari DewiОценок пока нет
- De Nition: Chapter 16 Blood PressureДокумент5 страницDe Nition: Chapter 16 Blood PressureAdebayo WasiuОценок пока нет
- Case 2 SlosДокумент7 страницCase 2 SlosNamarОценок пока нет
- Heart FailureДокумент29 страницHeart Failuremerin sunilОценок пока нет
- 1077 CMCNCHДокумент11 страниц1077 CMCNCHمحمد عقيليОценок пока нет
- Heart Failure and AnaesthesiaДокумент7 страницHeart Failure and AnaesthesiaShinta RizkyОценок пока нет
- Sic CHFДокумент2 страницыSic CHFPaolo TevesОценок пока нет
- PR ThoraksДокумент19 страницPR ThoraksKevin KarimОценок пока нет
- Defining Hemodynamic InstabilityДокумент9 страницDefining Hemodynamic InstabilitynadyajondriОценок пока нет
- HipotensiДокумент12 страницHipotensiAfdhalia Khairunnisa SyammarhanОценок пока нет
- Chapter 66 NotesДокумент16 страницChapter 66 NotesAlyssa Van VarkОценок пока нет
- Cardiogenic Shock Workup (Medscape)Документ8 страницCardiogenic Shock Workup (Medscape)Tia WasrilОценок пока нет
- G1-2. Clinical Applications - Persistent HypotensionДокумент1 страницаG1-2. Clinical Applications - Persistent Hypotensionj.jk.jk.17Оценок пока нет
- Interpretation CVP Measurements: Vol26 I971Документ7 страницInterpretation CVP Measurements: Vol26 I971AsmaahammadОценок пока нет
- Cirrhotic Cardiomyopathy: A Pathophysiological Review of Circulatory Dysfunction in Liver DiseaseДокумент8 страницCirrhotic Cardiomyopathy: A Pathophysiological Review of Circulatory Dysfunction in Liver DiseasecindyОценок пока нет
- Hypertension: SMF Saraf Rsud Bangli Fakultas Kedokteran Universitas Islam Al-Azhar 2018Документ49 страницHypertension: SMF Saraf Rsud Bangli Fakultas Kedokteran Universitas Islam Al-Azhar 2018Muhammad HidayatullahОценок пока нет
- Hypotension: Sandeep Sharma Priyanka T. BhattacharyaДокумент10 страницHypotension: Sandeep Sharma Priyanka T. Bhattacharyaمحمود محمدОценок пока нет
- ShockДокумент11 страницShockNatalia WiryantoОценок пока нет
- Hypertensive Emergency PDFДокумент14 страницHypertensive Emergency PDFOsiithaa CañaszОценок пока нет
- Cardiogenic Shock PDFДокумент14 страницCardiogenic Shock PDFAdreiTheTripleAОценок пока нет
- KGD 1 VivianДокумент101 страницаKGD 1 VivianVivian SaputraОценок пока нет
- Hypovolemic ShockДокумент10 страницHypovolemic ShockUsran Ali BubinОценок пока нет
- Current Strategies For The Prehospital Care of Congestive Heart FailureДокумент8 страницCurrent Strategies For The Prehospital Care of Congestive Heart FailureAmy Milligan MillerОценок пока нет
- Evaluation and Management of Elevated Intracranial Pressure in Adults - UpToDateДокумент41 страницаEvaluation and Management of Elevated Intracranial Pressure in Adults - UpToDateManuelEduardoSanchezSotoОценок пока нет
- Suae 023Документ6 страницSuae 023laac5757Оценок пока нет
- CardioДокумент9 страницCardioKESLING KAB. PANGANDARANОценок пока нет
- Cardiac TamponadeДокумент3 страницыCardiac TamponadeKimberly SolisОценок пока нет
- Cardiogenic Shock: Submitted ToДокумент5 страницCardiogenic Shock: Submitted Toal-obinay shereenОценок пока нет
- PRIN PBL Week 11 Tutorial 1Документ3 страницыPRIN PBL Week 11 Tutorial 1jonx225Оценок пока нет
- 8 Management of ShockДокумент8 страниц8 Management of ShockiisisiisОценок пока нет
- داتا حيداشر محاضرة فسيولوجىДокумент6 страницداتا حيداشر محاضرة فسيولوجىMohaned MokhtarОценок пока нет
- 2007 Vol2 (5) No1 pg56-64Документ9 страниц2007 Vol2 (5) No1 pg56-64Vebby 'bee' AstriОценок пока нет
- Smith Intracranial HypertensionДокумент55 страницSmith Intracranial HypertensionElena-Dana OpreaОценок пока нет
- Intensive Care Unit Arrhythmias: S.M. HollenbergДокумент13 страницIntensive Care Unit Arrhythmias: S.M. HollenbergEvita FebriyantiОценок пока нет
- Practice Essentials: Signs and SymptomsДокумент17 страницPractice Essentials: Signs and Symptomsdwi rizky kurniatiОценок пока нет
- Although Shock Has Been Recognised For Over 100 YearsДокумент4 страницыAlthough Shock Has Been Recognised For Over 100 YearsRusty HoganОценок пока нет
- PresentationДокумент13 страницPresentationLohcchana MoganОценок пока нет
- Fisiopatología Shock 1980Документ12 страницFisiopatología Shock 1980Alejo ZubietaОценок пока нет
- Dar o No Dar Fluidos 2012Документ8 страницDar o No Dar Fluidos 2012césar_campos_45Оценок пока нет
- Pt's ECG: Sinus Tachycardia, Left Axis Deviation, Anterolateral Wall IschemiaДокумент3 страницыPt's ECG: Sinus Tachycardia, Left Axis Deviation, Anterolateral Wall IschemiaKaiken DukeОценок пока нет
- Blood Flows, Pressure N ResistanceДокумент5 страницBlood Flows, Pressure N Resistancemaxwell amponsahОценок пока нет
- Cardiovascular and Autonomic Influences On Blood Pressure: John E. Jones,, Aruna R. Natarajan,,, and Pedro A. JoseДокумент23 страницыCardiovascular and Autonomic Influences On Blood Pressure: John E. Jones,, Aruna R. Natarajan,,, and Pedro A. JoseLulu LuwiiОценок пока нет
- Controlled HypotensionДокумент21 страницаControlled HypotensionChristian YonathanОценок пока нет
- ShockДокумент9 страницShockapocruОценок пока нет
- Acute Heart FailureДокумент9 страницAcute Heart FailureChen Briones100% (1)
- Congestive Heart Failure: Diagnosis, Pathophysiology, Therapy, and Implications For Respiratory CareДокумент10 страницCongestive Heart Failure: Diagnosis, Pathophysiology, Therapy, and Implications For Respiratory CareKevinDilianSugandaОценок пока нет
- Cardiac Tamponade and ManagementДокумент42 страницыCardiac Tamponade and Managementأم حمدОценок пока нет
- Chronic Heart FailureДокумент11 страницChronic Heart FailurelaydyОценок пока нет
- Jurnal FisioДокумент8 страницJurnal Fisiorizkya amanahОценок пока нет
- Post-Cardiac Arrest Management in Adults - UpToDateДокумент34 страницыPost-Cardiac Arrest Management in Adults - UpToDatehatsune100% (1)
- Shock and Critical Care: Presented BY: Palwasha KhanДокумент23 страницыShock and Critical Care: Presented BY: Palwasha KhanPalwasha KhanОценок пока нет
- Cardiopulmonary Cerebral ResuscitationДокумент17 страницCardiopulmonary Cerebral ResuscitationrizalОценок пока нет
- Clinmed 21 3 E275Документ8 страницClinmed 21 3 E275Carlos CoronaОценок пока нет
- Evaluation and Management of Elevated Intracranial Pressure in AdultsДокумент28 страницEvaluation and Management of Elevated Intracranial Pressure in AdultssandykumalaОценок пока нет
- S. 14.0 Fluid Therapy - Trauma CasesДокумент7 страницS. 14.0 Fluid Therapy - Trauma CasesroropujiОценок пока нет
- Edema Cerebral UPTODATEДокумент32 страницыEdema Cerebral UPTODATEChristian Andres Cruz PerezОценок пока нет
- Braunwald: Chronic Coronary Artery DiseaseДокумент122 страницыBraunwald: Chronic Coronary Artery Diseaseusfcards100% (1)
- Lecture 7.2 Lipid MetabolismДокумент8 страницLecture 7.2 Lipid MetabolismHuzaifa MehmoodОценок пока нет
- Diabetes Mellitus Type 2Документ23 страницыDiabetes Mellitus Type 2Jennifer CastilloОценок пока нет
- Muscle CrosswordДокумент3 страницыMuscle CrosswordStasia CleggОценок пока нет
- ABC of Clinical Electrocardiography Myocardial IschaemiaДокумент6 страницABC of Clinical Electrocardiography Myocardial IschaemiaShri Mahalaxmi HarishОценок пока нет
- Electrolytes: Regulation of Body Fluid CompartmentsДокумент6 страницElectrolytes: Regulation of Body Fluid Compartmentsbuhari rabiuОценок пока нет
- Predisposing Factors: Age Neurological Condition Immunity Precipitating Factors: Smoking Environment LifestyleДокумент2 страницыPredisposing Factors: Age Neurological Condition Immunity Precipitating Factors: Smoking Environment LifestyleDavid RefuncionОценок пока нет
- Fundamentals of NursingДокумент27 страницFundamentals of NursingRobeth OrbisoОценок пока нет
- Microlife BP A1 Easy N-V9 1520Документ61 страницаMicrolife BP A1 Easy N-V9 1520EdvinasОценок пока нет
- Englishfile 4e Upperintermediate Teachers Guide1Документ7 страницEnglishfile 4e Upperintermediate Teachers Guide1abasОценок пока нет
- Intro To Computational NeuroscienceДокумент156 страницIntro To Computational NeuroscienceMohammad Haikal bin Mohammad IsaОценок пока нет
- Science6 q2 Mod3 Explain How The Different Organ System v2Документ28 страницScience6 q2 Mod3 Explain How The Different Organ System v2Mark James VallejosОценок пока нет
- The Renal SystemДокумент10 страницThe Renal SystemWahyu Purbo PangestiОценок пока нет
- Pulse Oximetry - UpToDate PDFДокумент26 страницPulse Oximetry - UpToDate PDFLOIDA ESTHER DIAZ MONTESОценок пока нет
- Final Project - Vanessa Fuerstenberg P.2Документ9 страницFinal Project - Vanessa Fuerstenberg P.2nessaОценок пока нет
- Mechanical Ventilation - Initial SettingsДокумент57 страницMechanical Ventilation - Initial SettingsabdallahОценок пока нет
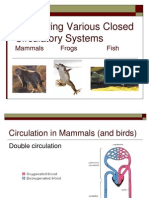
- Comparing Various Closed Circulatory Systems: Mammals Frogs FishДокумент12 страницComparing Various Closed Circulatory Systems: Mammals Frogs Fishrishadabubecker100% (1)
- DIPASREE - ROYCHOWDHURYAnomalous Secondary Growth in Boerhaavia Stem2020!04!03Anomalous Secondary Growth in Boerhaavia StemДокумент2 страницыDIPASREE - ROYCHOWDHURYAnomalous Secondary Growth in Boerhaavia Stem2020!04!03Anomalous Secondary Growth in Boerhaavia StemAkshay KannanОценок пока нет
- Clinical Cheat Sheet: Radiographic AssessmentДокумент1 страницаClinical Cheat Sheet: Radiographic AssessmentTracy PopeОценок пока нет
- Physiology-Summary NotesДокумент201 страницаPhysiology-Summary NotesReem NasserОценок пока нет
- Bath and Dress Infants and ToddlersДокумент16 страницBath and Dress Infants and ToddlersJohn Paolo AladОценок пока нет
- Psych 133 SyllabusДокумент5 страницPsych 133 SyllabusRushil SurapaneniОценок пока нет
- MPAH SCДокумент3 страницыMPAH SCBernard ChanОценок пока нет
- Physio Xtra Slides Color 2021Документ17 страницPhysio Xtra Slides Color 2021teapalmtreeОценок пока нет
- Cardiotonics & Inotropic Drugs PDFДокумент10 страницCardiotonics & Inotropic Drugs PDFZehra AmirОценок пока нет
- MS LAB Oxygenation Nursing SkillsДокумент9 страницMS LAB Oxygenation Nursing SkillsRouwi DesiatcoОценок пока нет
- Volibris MOA Storyboard v1 1Документ4 страницыVolibris MOA Storyboard v1 1shyamchepurОценок пока нет