Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Youre Only Old Once A Book For Obsolete - DR SeussДокумент29 страницYoure Only Old Once A Book For Obsolete - DR Seussborysanselmo15% (26)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Apex Predator DietДокумент73 страницыThe Apex Predator Dietdeclanku100% (2)
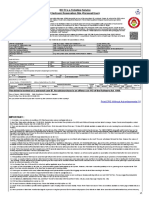
- Train Ticket PDFДокумент2 страницыTrain Ticket PDFVarun Kumar Akula100% (1)
- 6 Week Fat Crusher Plan PDFДокумент39 страниц6 Week Fat Crusher Plan PDFȘtefania Camelia HorvathОценок пока нет
- Commissioning and Qualification ASTM ApproachДокумент0 страницCommissioning and Qualification ASTM Approachvenki_beeОценок пока нет
- Catfish Farming Information Guide - AgrifarmingДокумент5 страницCatfish Farming Information Guide - AgrifarmingamolkajaleОценок пока нет
- Sitxfsa002, Sitxinv002 - Written Assessment v2Документ24 страницыSitxfsa002, Sitxinv002 - Written Assessment v2hazem khudair100% (1)
- F & B Cost Control: Professional Chefs AssociationДокумент9 страницF & B Cost Control: Professional Chefs AssociationOtpor Stoko100% (1)
- Article On ButterflyДокумент1 страницаArticle On ButterflyLalaijuhОценок пока нет
- Karakteristik Lactobacillus Spesies Yang Diisolasi Dari Daging SapiДокумент5 страницKarakteristik Lactobacillus Spesies Yang Diisolasi Dari Daging SapiSyahrul HidayatОценок пока нет
- The Combined Influence of Temperature and Modified Atmospheres On Tribolium Castaneum (Herbst) (Coleoptera Tenebrionidae)Документ8 страницThe Combined Influence of Temperature and Modified Atmospheres On Tribolium Castaneum (Herbst) (Coleoptera Tenebrionidae)Maurício de OliveiraОценок пока нет
- 463 Quantifiers 2 Test A1 A2 Grammar ExercisesДокумент3 страницы463 Quantifiers 2 Test A1 A2 Grammar ExercisesRiyad SiddiqueОценок пока нет
- Moawia ElBerier Manufacturing PLCДокумент9 страницMoawia ElBerier Manufacturing PLCAsmaa MoawiaОценок пока нет
- Jelena Pjescic RESUMEДокумент1 страницаJelena Pjescic RESUMEЈелена КошевићОценок пока нет
- Reading Comprehension 1Документ5 страницReading Comprehension 1Abilashini KumarОценок пока нет
- Voh 11Документ19 страницVoh 11Siphiwe Christopher MathebulaОценок пока нет
- Step 1: Recognize Your Strengths: Executive SummeryДокумент8 страницStep 1: Recognize Your Strengths: Executive SummeryOwais JavedОценок пока нет
- Akili Exams. The Wings of ExcellenceДокумент16 страницAkili Exams. The Wings of ExcellenceDoreen Benezeth100% (2)
- Final Research PaperДокумент12 страницFinal Research PapermargiОценок пока нет
- Cookery VS CulinaryДокумент4 страницыCookery VS CulinaryJuli Hyla RomanoОценок пока нет
- p2 Science Food Webs Lesson g5Документ5 страницp2 Science Food Webs Lesson g5api-358299697Оценок пока нет
- 209 469 1 SMДокумент7 страниц209 469 1 SMpandhegaОценок пока нет
- Bull Semen Collection and Analysis For ArtificialДокумент11 страницBull Semen Collection and Analysis For ArtificialAdleend RandabungaОценок пока нет
- Case Study - How An Effective Manager Handles Precarious Situations "Left or Right"Документ1 страницаCase Study - How An Effective Manager Handles Precarious Situations "Left or Right"VAIDIK JOSHIОценок пока нет
- Food Adulteration and Its Quick TestДокумент17 страницFood Adulteration and Its Quick TestZubair AbidОценок пока нет
- Animal Aid USA To Join Chow Hounds Food Distribution Project in Camden June 8thДокумент2 страницыAnimal Aid USA To Join Chow Hounds Food Distribution Project in Camden June 8thanimalaidusaОценок пока нет
- Volume 14 Nomor 2 September 2013-Zubaidah PENINGKATAN PERTUMBUHAN DAN HASIL JAMUR TIRAM (Pleurotus Ostreatus) MELALUI VARIASI KOMPOSISI MEDIA TANAMДокумент8 страницVolume 14 Nomor 2 September 2013-Zubaidah PENINGKATAN PERTUMBUHAN DAN HASIL JAMUR TIRAM (Pleurotus Ostreatus) MELALUI VARIASI KOMPOSISI MEDIA TANAMJurnal Ilmiah Agri peat FAPERTA UNPARОценок пока нет
- 03 Life Processes Chapter Wise Important QuestionsДокумент17 страниц03 Life Processes Chapter Wise Important Questionsmm8871100% (1)
- Ceasars Salad With Shredded Chicken: Sauce For 20 PaxДокумент3 страницыCeasars Salad With Shredded Chicken: Sauce For 20 PaxDwita HarahapОценок пока нет
- School Lunch Parents SurveyДокумент2 страницыSchool Lunch Parents Surveyapi-199453431Оценок пока нет